Higher Prepregnancy BMI Category Linked to Increase in Poor Maternal and Neonatal Outcomes
Women with class 3 obesity before becoming pregnant have up to a 4.5-fold greater risk of composite maternal morbidity that includes preeclampsia, preterm delivery, DM.
Increase in prepregnancy class of body mass index (BMI) was associated with a corresponding and significant increase in the odds of composite pregnancy morbidity that rose to 4.4-fold higher for women with class 3 obesity compared to those with average prepregnancy BMI, according to a new study that included more than 40 000 pregnant women.1


©Kletter/Shutterstock.com

Authors of the retrospective cohort analysis reported a parallel increase in composite neonatal morbidity with increasing maternal BMI that included hypoglycemia, respiratory distress syndrome, and APGAR score of less than 7 at 5 minutes postpartum.
The long-term health consequences of obesity are well-known but study authors, writing in the Journal of Osteopathic Medicine, stress that research on the impact of obesity on reproductive-aged and pregnant women has been affected by poor study design including failure to assess associated risk by specific maternal class of obesity; assessment of BMI at time of delivery; use of billing codes alone to measure outcomes; and assessment of birthweight alone as a measure of BMI impact on outcomes.1
Citing data that show more than 1 in 3 women in the United States have overweight and that more than 50% of pregnant women have overweight or obesity,2 the researchers stated, "It is necessary to clearly understand the extent to which BMI affects pregnancy morbidity so that mitigation strategies can be appropriately employed preconception."1
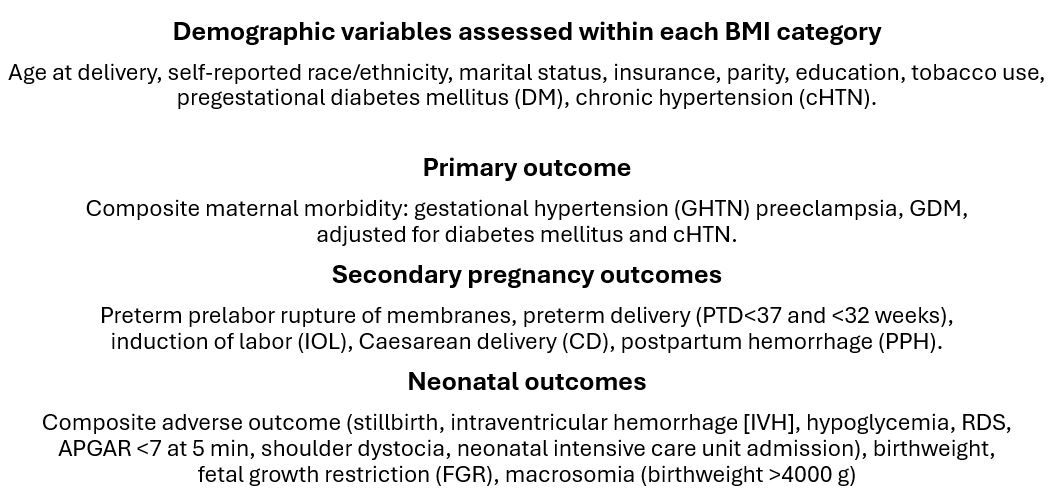
For their retrospective analysis, senior author Kajal Angras, DO, from the Department of Obstetrics and Gynecology, Geisinger Health System, in Danville, PA, and colleagues tapped data for pregnant women who delivered singleton births within the 5 delivery hospitals in the Geisinger Health System in Pennsylvania between October 2007 and December 2023, including all pregnancies in which maternal prepregnancy BMI was 18.5 kg/m2 or greater. They assessed risk of pregnancy and neonatal morbidity by maternal prepregnancy BMI category, ie, normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and class 1 (30.0–34.9 kg/m2), class 2 (35.0–39.9 kg/m2), and class 3 (40.0 kg/m2 and greater) obesity. Demographic variables assessed and the primary and secondary outcomes for pregnant women and neonates follow1:


FINDINGS1
Of the 40 256 pregnant women with 55 202 singleton pregnancies identified, data on 53 664 neonates were available for analysis. Angras et al reported the cohort BMI categories as follows: 32% normal weight, 26.1% overweight, 16.8% class 1 obesity, 103% class 2 obesity, and 8.6% class 3 obesity. The mean participant age at delivery was 28.5 years and the majority of participants (79.7%) identified as non-Hispanic White.
After investigators controlled for potential confounders, they observed statistically significant increasing odds ratios (ORs) across BMI classes for several adverse outcomes. Odds (95% CI) of composite maternal morbidity were 1.72 (1.63-1.82) for overweight, 2.66 (2.50-2.84) for class 1 obesity, 3.35 (3.08-3.65) for class 2 obesity and 4.4 (3.70-5.22) for class 3 obesity (P < .01 for all). Risk for GHTN increased to a similarly alarming level as BMI category increased, with 4.5-fold greater odds (OR 4.55 (3.67-5.63; P < .01) conferred by class 3 obesity.
Compared with participants who maintained a normal prepregnancy BMI, results showed that those with any class of obesity faced a greater risk of hypertensive disorders of pregnancy and GDM. In the subgroup of participants with class 3 obesity, in addition to the 4-fold increased risk of GHTN, Angras and colleagues found the risk of developing preeclampsia was more than doubled (OR 2.35) and of GDM nearly doubled (OR 1.71). (P < .01 for all).
According to the study, the odds of IOL, CD, PTD less than 32 weeks, and PPH also increased in step with increase in obesity class. Conversely the analysis revealed a protective effect for FGTR.
Composite neonatal morbidity also increased with increase in maternal BMI class, with an OR of 1.47 (1.28-1.69) for mothers with class 3 obesity. The risk for neonatal hypoglycemia increased to 1.73 (1.42-2.12) in the class 3 obesity group. (P < .01 for all). Investigators noted the increase in odds of macrosomia, calling the 1.63 increased odds of a macrosomic infant for those with even class 2 obesity a “clinically relevant” finding. Moreover, participants with any class of obesity faced greater risk of all neonatal outcomes of interest, the researchers stressed.
“While it seems intuitive that patients with class III obesity would be at the highest risk for adverse outcomes, this is one of the larger studies in the United States assessing these outcomes for the individual classes based on prepregnancy BMI,” Angras and team wrote.1
Among the study limitations the authors note is the homogeneity of the study population as well as that composition’s effect on reducing the occurrence of some negative outcomes more often observed in racial and ethnic minority groups not represented. They caution that both drawbacks may limit the ability to generalize findings beyond the study cohort.
Those notes notwithstanding, the authors conclude that their findings “can be applied to help facilitate antenatal counseling of pregnant women” based on the BMI class-specific pregnancy outcomes observed.1
References
1. Mackeen AD, Boyd VE, Schuster M, Young AJ, Gray C, Angras K. The impact of prepregnancy body mass index on pregnancy and neonatal outcomes. J Osteopath Med. Published online May 16, 2024. doi:10.1515/jom-2024-0025
2. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief 2020;1–8. PMID: 32487284. https://www.cdc.gov/nchs/products/databriefs/db360.htm






Bringing PPD Screening to the Forefront of Maternal Health: A Q&A with Joy Baker, MD
June 3rd 2025ACOG 2025: Joy Baker, MD, discusses the urgent need to prioritize postpartum depression screening, normalize mental health in prenatal care, and strengthen continuity between OB-GYN and primary care.

