

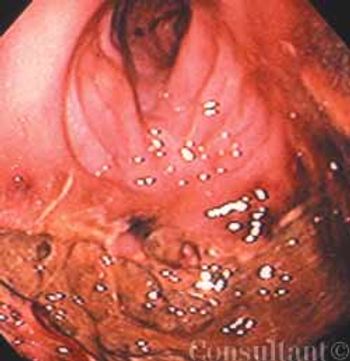
Endoscopic evaluation of a 61-year-old man hospitalized with a 4-month history of rectal bleeding, mucus discharge, and change in bowel habits revealed this large, sessile villous adenoma.
Endoscopic evaluation of a 61-year-old man hospitalized with a 4-month history of rectal bleeding, mucus discharge, and change in bowel habits revealed this large, sessile villous adenoma.

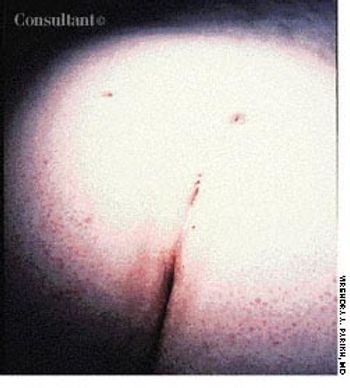
Following mechanical bowel preparation and prophylactic antibiotic therapy, a 59-year-old man underwent transanal excision of a villous adenoma of the distal rectum. Two weeks after discharge, he returned with a temperature of 38.9°C (102°F), abdominal pain, and diarrhea.

Ten days before presenting for evaluation, a 69-year-old man began to experience neuralgic pain and noticed the eruption of painful erythematous macules and papules on the right side of his chest. Within 24 to 72 hours, vesicles and pustules arose at the site. One week after onset, several of the lesions dried and crusted.

A 79-year-old male nursing home resident with Parkinson's disease was brought to the emergency department after 3 days of severe constipation and inability to pass flatus. Examination showed generalized abdominal distention with tympany. Results of rectal examination were normal.

For 2 months, a 73-year-old man had experienced dysuria, pneumaturia, and foul-smelling urine. He had an attack of diverticulitis a year earlier. At that time, he underwent a barium enema study, which showed multiple sigmoid colonic diverticula with spasm.

Endoscopic evaluation of a 61-year-old man hospitalized with a 4-month history of rectal bleeding, mucous discharge, and change in bowel habits revealed this large, sessile villous adenoma. The lesion occupied half the circumference of the bowel wall in the distal sigmoid colon, 25 cm from the anal verge. Examination of biopsy specimens showed benign villoglandular adenoma with atypia, with no invasive carcinoma. Sigmoid resection was carried out, and the patient recovered well.
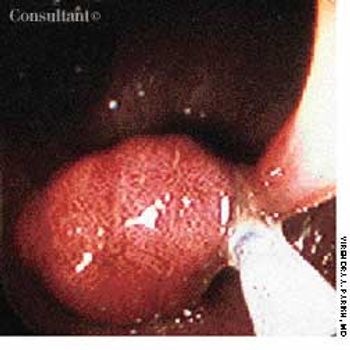
When a 59-year-old man's stool tested positive for occult blood, colonoscopic evaluation was carried out. This is the endoscopic appearance of a pedunculated colonic adenoma-the source of the bleeding-being removed by a snare.

For 3 days, a 69-year-old man had had intermittent colicky pain on the right side of the abdomen, loose bowel movements, and a low-grade fever. Examination disclosed a mildly tender, palpable, diffuse mass in the right upper quadrant and hyperactive bowel sounds. The patient's stool was positive for occult blood, and a complete blood cell count showed a low hemoglobin level and a slightly elevated white blood cell count.
Pain, swelling, and purulent, blood-stained drainage around the lower back had plagued a 21-year-old woman for 3 weeks. On examination, multiple openings were seen overlying the natal cleft, the sacrococcygeal region, and the upper part of the midline. The last was the area of drainage. Insertion of a metal probe at that point revealed a pilonidal sinus that communicated with centrally located openings.
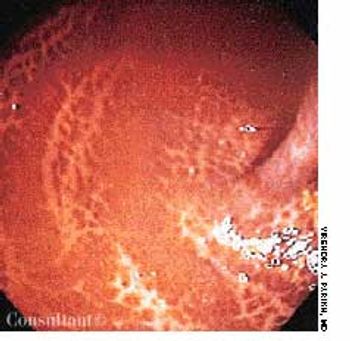
A 65-year-old woman had had diarrhea for 1 year. Stool studies were negative for occult blood, and flexible sigmoidoscopy revealed a cobblestone-patterned colonic mucosa. A detailed history revealed that for the past year, the patient had been taking a daily herbal multivitamin supplement, the ingredients of which included cascara. Her diarrhea resolved completely when she stopped taking the pills.
A 75-year-old obese woman with subacute-onset dyspnea and lower right posterior chest pain was brought to the emergency department. She had a history of diastolic heart failure, arthritis, and suspected obstructive sleep apnea. The patient was dyspneic at rest.
A 73-year-old man with chronic constipation presented to the emergency department with hematochezia. Mild, colicky abdominal pain had begun 3 days earlier; obstipation had been present for 10 days.The patient’s history included a cerebrovascular accident 2 years earlier and Parkinson disease; he was taking anticholinergic drugs.

A 74-year-old woman was admitted to the hospital with abdominal pain, weight loss, fatigue, and change in bowel habits of 6 months’ duration. Her hemoglobin level was 7 g/dL; carcinoembryonic antigen, 672 ng/dL.

A 48-year-old woman complained of dull, aching abdominal pain and epigastric swelling. She had a 6- to 7-month history of painless swelling that intermittently decreased in size. The patient denied vomiting and nausea.
An obese 55-year-old woman had intermittent dysuria and frequent urination for 4 days and fever, abdominal pain, and vomiting for 3 days. Her history included type 1 diabetes mellitus, hypertension, and angina; her medications included insulin, nifedipine, and nitroglycerin.

Progressive abdominal distention, nausea, constipation, and mild abdominal pain developed in an 82-year-old woman 5 days after she underwent surgical repair of a left hip fracture. Her medical history was significant for Parkinson disease, type 2 diabetes mellitus, and hypertension.

During surgical resection for colon cancer, an 8.5-cm diverticulum was found incidentally in a 70-year-old man. The lesion arose from the antimesenteric surface of the terminal ileum; it was located about 2 ft proximal to the ileocecal junction. Palpation of the diverticulum revealed a hard mass at its tip and a thickened wall at its base.
A 26-year-old woman complained of flatus and fecal incontinence of solid stool.One year earlier, she was delivered of a 3.86-kg (8.5-lb) infant; a severe perinealtear was repaired after the birth.

A 75-year-old woman had a 1-year history of an anal protrusion, bloodstained mucus discharge, and anal incontinence of flatus and loose stools.

April 11th 2011

September 14th 2005

September 14th 2005

September 14th 2005

September 14th 2005

September 14th 2005