Articles by Hesham Taha, MD

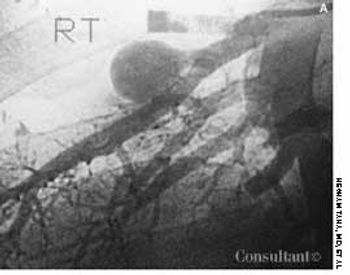
Frequent urinary tract infections and unexplained hypertension (160/100 mm Hg) occurred in a 38-year-old man with no significant medical history. The heart and chest were normal; a right lower quadrant mass was detected in the abdomen. Red blood cells were found in the urine. An abdominal CT scan demonstrated that the left kidney was fused to the lower pole of the right kidney with the left pelvicaliceal system to the left of the midline; these findings are consistent with crossed fused renal ectopia. Cystographic and cystoscopic examinations were normal.

An 80-year-old woman presented with recurrent abdominal pain for 1 month, constipation, and vomiting. She had no diarrhea, rectal bleeding, or weight loss.
A 28-year-old woman reported that she was in good health before experiencing generalized weakness; exhaustion; and pain in her legs, shoulders, and back for the past 3 months. She also complained of shortness of breath with minimal activity, irregular menstrual periods, and occasional episodes of nose and gum bleeding.

Back pain and weakness of both legs had bothered this 60-year-old woman for 1 week. Left breast cancer, stage 2, had been diagnosed 2 years before, and subsequently she underwent a lumpectomy followed by chemotherapy and radiation therapy.
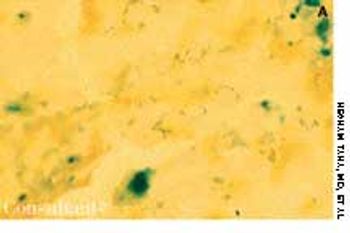
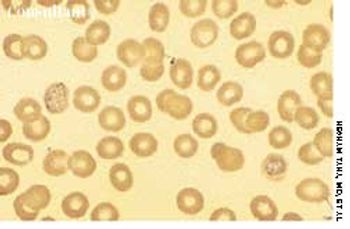
A 70-year-old woman with a history of ischemic heart disease was hospitalized because of generalized weakness, fatigue, and retrosternal chest pain on mild exertion. Her skin was pallid. Chest and heart evaluations were normal, and mild hepatosplenomegaly was discerned.

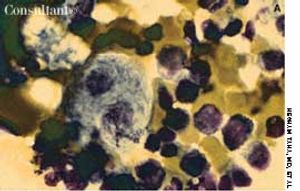
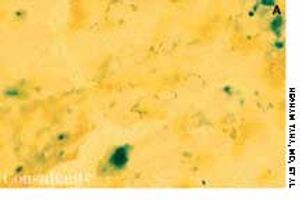
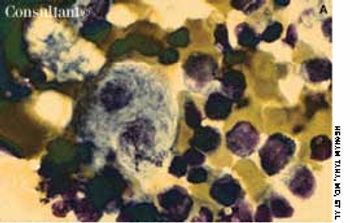
Sézary Syndrome
ByHesham Taha, MD,Japinder Singh, MD,Gamil Kostandy, MD,Osama Ayad, MD,Maged Ghaly, MD,David Dosik, MD A 55-year-old woman with no significant medical history reported that diffuse erythematous, patchy, purpuric skin lesions over most of her body had been present for the past year. Applications of an over-the-counter corticosteroid cream helped control the pruritus but did not clear the skin lesions.

A 46-year-old woman sought treatment of vaginal pruritus of 6 months' duration. She also was bothered by generalized skeletal aching that was most prominent in her legs. The patient had a history of hypertension.

A 66-year-old man presented to the emergency department complaining of vomiting “coffee ground” emesis for 3 days. His history revealed chronic alcoholism for the last 30 years.

A 50-year-old man with a history of diabetes, hypertension, seizure disorder, and alcohol abuse sought treatment for a rash and painful ulcerations of the hand, face, and scalp, which had bothered him for 1 month. The patient also complained of pruritus.
A 20-year-old woman, who had been confused and delirious for 2 days, was brought to the emergency department (ED). She had no significant past medical history and was taking no medication but had recently returned from a trip to Southeast Asia. In the ED, the patient had several convulsions and rapidly became comatose. She was unresponsive; her temperature was 37.9°C (100.3°F), and her blood pressure measured 80/50 mm Hg. The neurologic examination showed no signs of meningeal irritation. Cranial nerve examination was normal and showed mild, bilateral, symmetric increase in deep tendon reflexes. All other physical examination findings were normal.
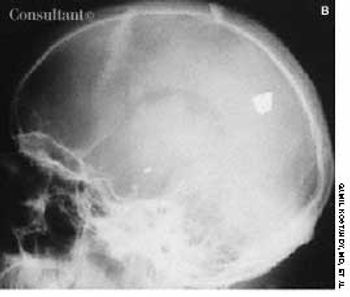
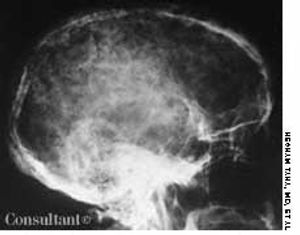
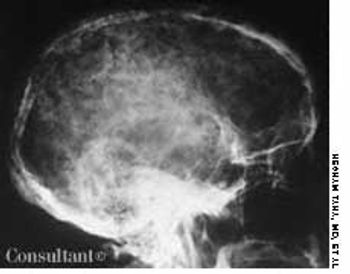
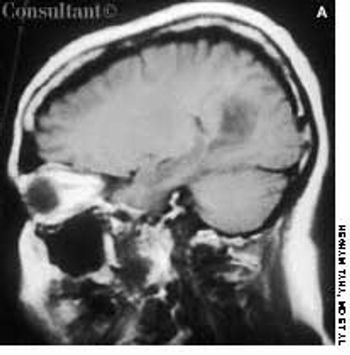
Bullet in the Brain
ByGamil Kostandy, MD,Hesham Taha, MD,Salama Salama, MD,Maged Ghaly, MD,Bruce Sosler, MD,Hani Ashamalla, MD While evaluating this 26-year-old man for suspected sinusitis, skull films revealed the fragments of a 32-caliber gunshot embedded in his brain. The anteroposterior and lateral radiographs show three metallic bullet fragments; the largest remnant is on the left side of the occipitoparietal region. The patient reported being shot at age 11 but denied any residual neurologic signs.
Headache and vomiting suddenly developed in a 41-year-old woman who was 16 weeks pregnant. The next day, she suffered an episode of tonic-clonic seizures associated with a 15-minute loss of consciousness.
A 22-year-old man complained of progressive shortness of breath and abdominal distention. Three years before, he had completed chemotherapy for Hodgkin's disease and had since been in remission. Recently, he had been treated for tonsillitis with oral antibiotics.

A 40-year-old woman was concerned about an area of redness and tenderness on her left breast. Despite antibiotic therapy prescribed by another physician, the rash had progressed during the past month to erythema and nodules that involved the anterior chest and right breast.
A 65-year-old man with no significant medical history presented with mild abdominal pain-primarily in the left lower quadrant-and bleeding gums. He had a petechial rash over the entire body and hepatosplenomegaly 10 cm below the costal margin.