
























































































































































The key factor in reducing morbidity and mortality in patients with chronic obstructive pulmonary disease (COPD) continues to be smoking cessation. Newer formulations of nicotine replacement therapy-a nasal spray and an inhaler-provide rapid delivery of nicotine and may be appropriate for highly dependent smokers. Bupropion has been shown to improve smoking cessation rates, either when used alone or with a nicotine patch. Both the influenza and pneumococcal vaccines are recommended to reduce the morbidity and mortality associated with respiratory infections in patients with COPD.
Sleep Disorders
Latest News
Advertisement
Advertisement
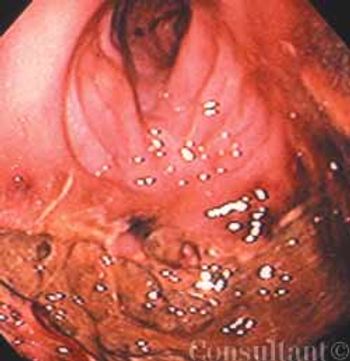
A 75-year-old obese woman with subacute-onset dyspnea and lower right posterior chest pain was brought to the emergency department. She had a history of diastolic heart failure, arthritis, and suspected obstructive sleep apnea. The patient was dyspneic at rest.
ABSTRACT: A cough is considered chronic when it persists for 3 or more weeks. Typically, chronic cough is a lingering manifestation of a viral upper respiratory tract infection; other, more serious causes-such as asthma, sinusitis, or gastro- esophageal reflux-must also be considered. Look to the history for diagnostic clues and order a chest film, which may point to pneumonia, hyperinflation, atelectasis, or cardiac or pulmonary abnormality. Diagnostic test methods will depend, in part, on the child's age; for example, the American Academy of Pediatrics recommends against imaging of the sinuses in children 6 years or younger. Pulmonary function tests can be useful in diagnosing asthma if the child is able to cooperate. Consider ordering a barium swallow for a very young child whose cough may be the result of a vascular anomaly. A pH probe study can help you determine whether cough is secondary to gastroesophageal reflux. Treatment is directed at the underlying cause.
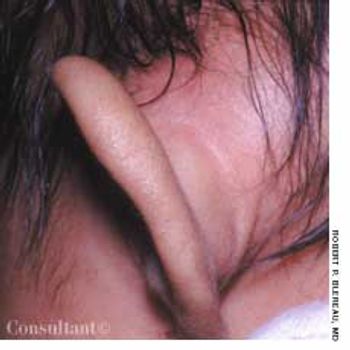
Concerned that her 7-week-old daughter's left ear was far more prominent than the right one, the mother took the infant to the emergency department (ED) for evaluation. The swelling had begun 3 or 4 days earlier; the patient was otherwise asymptomatic.
ABSTRACT: The results of diagnostic tests do not correlate well with the presence and severity of pain. To avoid missing a serious underlying condition, look for "red flags," such as unexplained weight loss or acute bladder or bowel function changes in a patient with low back pain. Nonopioid medications can be more effective than opioids for certain types of pain (for example, antidepressants or anticonvulsants for neuropathic pain). When NSAIDs are indicated, cyclooxygenase-2 inhibitors are better choices for patients who are at risk for GI problems or who are receiving anticoagulants. However, if nonspecific NSAIDs are not contraindicated, consider using these far less expensive agents. The tricyclic antidepressants are more effective as analgesics than selective serotonin reuptake inhibitors. When opioids are indicated, start with less potent agents (tramadol, codeine, oxycodone, hydrocodone) and then progress to stronger ones (hydromorphone, fentanyl, methadone, morphine) if needed.
In general, asthma-related morbidity and mortality are greatest among members of ethnic minority groups who live in the inner cities; about 5000 deaths occur in these populations each year in the United States.
A 12-year-old African American girl comes to youroffice for a well-child checkup. She is tall for herage (height above the 95th percentile) and obese(body mass index [BMI] above the 95th percentile).Physical examination reveals acanthosisnigricans on her neck, axilla, and upper abdominalregion (Figure) and a vaginal yeast infection.Routine urinalysis reveals a glucose level ofgreater than 1000 mg/dL, with negative proteinand ketones. A random blood glucose test, obtainedbecause of the glucosuria, is 249 mg/dL.
ABSTRACT: Once you have excluded a cardiac origin of chest pain, focus the evaluation on esophageal, psychiatric, musculoskeletal, and pulmonary causes. Gastroesophageal reflux disease (GERD) and esophageal motility disorders are the most common causes of unexplained chest pain (UCP). If you suspect an esophageal disorder, empiric antisecretory therapy is the most cost-effective initial approach. If the patient remains symptomatic, order a 24-hour esophageal pH study with symptom analysis while the patient receives maximal acid suppression. Once GERD is excluded, the patient may be treated for visceral hyperalgesia with low-dose tricyclic antidepressants or standard doses of selective serotonin reuptake inhibitors. Panic disorder-the most common psychiatric disorder in patients with UCP-is often associated with atypical symptoms, such as palpitations and paresthesias, and other psychiatric disorders. If you suspect panic disorder, one approach is to give the patient a short-term, nonrefillable prescription for a benzodiazepine and refer him or her for psychiatric evaluation.
ABSTRACT: Fibromyalgia syndrome (FMS) is a common condition that causes chronic pain and disability. It should be diagnosed by its own clinical characteristics of widespread musculoskeletal pain and multiple tender points. American College of Rheumatology criteria guidelines are most helpful in diagnosing FMS. The major symptoms are pain, stiffness, fatigue, poor sleep, and those of other associated conditions, for example, irritable bowel syndrome, headaches, restless legs syndrome, chronic fatigue syndrome, and depression. The pathophysiology of FMS is thought to involve central sensitization and neuroendocrine aberrations, triggered or aggravated by genetic predisposition; trauma; psychosocial distress; sleep deprivation; and peripheral nociception.
ABSTRACT: Many patients with presumed mild intermittent asthma have unrecognized persistent symptoms; these can be elicited with specific questioning about coughing, wheezing, shortness of breath, chest tightness, nighttime awakenings, and exercise intolerance. Asthma severity may vary with the season. For asthmatic patients with predictable seasonal allergies, prescribe inhaled corticosteroids for a few weeks or months beginning 2 to 3 weeks before usual symptom onset. Successful long-term management requires identification and control of asthma triggers, such as cigarette smoke, house dust mites, cockroaches, molds, and animal dander. Removing triggers or minimizing the patient's exposure to them may allow improved asthma control with lower dosages of corticosteroids.
Consider a concentrated solution(10 mg/mL) of doxepin for patientswith fibromyalgia who experienceside effects with other tricyclics ateven 10-mg doses.
ABSTRACT: Effective smoking cessation strategies typically encompass the use of some pharmacotherapy with counseling by physicians. Give the Fagerstrom test to patients who want to quit smoking to determine their degree of nicotine dependence. For low-nicotine-dependent smokers, the use of 1 smoking cessation product for a short period has proved successful; for high-dependence smokers, a combination of products, such as nicotine gum and a nicotine patch, can be used. Other available smoking cessation products are the nicotine nasal spray, the nicotine inhaler, and sustained-release bupropion. Increasing the dose or duration of nicotine gum and patch has improved abstinence rates among high- dependence smokers. Quit rates have also been shown to increase with the dose of bupropion.
The Geriatric Depression Scale is the most widelyvalidated screening tool. The questionnaire has beenreduced to a single question that is as sensitive and as specificas the 15-item shortened form of the original 30-itemscale. The question is: "How often do you feel sad or depressed?'This is certainly something that is easy to ask inthe course of a general physical examination or routine officevisit.
ABSTRACT: Infant colic is a diagnosis of exclusion; its true cause is not known. To rule out alternative diagnoses, obtain a detailed history, look for clues to an underlying organic disease or genetic syndrome, and perform regular head-to-toe physical examinations. The interventions most commonly used to treat colic include modification of parental behavior (such as increased carrying of the infant or decreased infant stimulation), milk- and/or soy-free formulas, modifications in the diet of a breast-feeding mother, soothing measures (such as car rides, rocking, or use of a pacifier), anticholinergic agents, sedatives, and alternative medicine approaches (such as sucrose solution, herbal teas, or infant massage). The medications used to treat colic-such as antispasmodics and anticholinergics-can have serious adverse effects; discuss the pros and cons of drug therapy with parents before prescribing these agents. Remind parents that colic resolves by age 3 to 4 months, regardless of the intervention used.
Traditionally, urologists have cared for patients with benign prostatic hyperplasia (BPH). However, because of demographic fluctuations, changes in the health care system, and the development of effective pharmacologic therapy for BPH, primary care physicians are increasingly involved not only in initial patient evaluation but also in continuing management. Here we provide guidelines for treatment of uncomplicated BPH--with special emphasis on medical therapies.
Many patients who present to the emergency department(ED) with severe headache request a narcotic to relieve thepain.
A 34-year-old woman complains of headaches that interfere with work. Her first headache episode, approximately 6 yearsearlier, was relatively mild. Initially, she experienced attacks only once every 3 to 4 months and managed them effectivelywith over-the-counter (OTC) agents. However, in the last 6 months the attacks have become more frequent-they occur atleast twice a month-and are so severe that she misses work.
ABSTRACT: The most common errors in measuring blood pressure (BP) are using the incorrect cuff size, not having the patient relax for 5 minutes before the measurement, and deflating the cuff too quickly. Observer bias may compound technical errors. When patients use the proper procedure, home BP measurements may be more reproducible than office measurements. Brachial artery-based monitors are more accurate than finger- or wrist-based instruments. To ensure that patients measure their BP correctly, observe their technique with their own monitors. Counsel patients to measure their BP at predetermined times and to have their monitors validated periodically.
The diagnosis of osteoarthritis (OA) is primarily clinical. Key historical clues to idiopathic OA include patient age greater than 45 years, joint pain that increases with activity and is relieved with rest, morning stiffness of 30 minutes duration or less, and involvement of one or more of the following: hips, knees, cervical or lumbar spine, basilar thumb joints, interphalangeal joints of the hands, midfoot joints, and first metatarsophalangeal joints.
ABSTRACT: Topical agents can provide temporary relief from osteoarthritis symptoms with little or no risk. Acetaminophen is first-line oral therapy. Be alert for risk factors for NSAID-induced GI toxicity, such as concurrent use of prescription and OTC agents. Tramadol, narcotic analgesics, muscle relaxants, and antidepressants are options when NSAIDs are ineffective or contraindicated. Intra-articular injections of corticosteroids or hyaluronan are appropriate for patients who have a single joint exacerbation. Total knee and total hip arthroplasty are considered the most effective surgical interventions.
ABSTRACT: The main therapeutic goals for patients who have an acute coronary syndrome are to reestablish normal epicardial flow and to increase distal myocardial perfusion. Fibrinolytic treatment with tissue plasminogen activator within 70 minutes of the onset of symptoms dramatically reduces the mortality rate from myocardial infarction. Other fibrinolytic agents include reteplase, which is given as a double bolus, and tenecteplase, which is given as a single bolus. In most hospitals, fibrinolytic therapy is more readily available than percutaneous transluminal coronary angioplasty (PTCA); however, PTCA may be the preferred approach if it is available within an hour and a half. Antiplatelet drugs, such as glycoprotein IIb/IIIa receptor antagonists, are used to improve distal myocardial perfusion. If follow-up coronary angiography is not available to assess whether epicardial blood flow and distal myocardial perfusion have been restored, a 12-lead ECG can provide valuable information. The resolution of ST-segment abnormalities is a marker for improved perfusion.
ABSTRACT: Unless the cause of back pain is obvious, order anteroposterior and lateral radiographs of the spine, a complete blood cell count, erythrocyte sedimentation rate, and urinalysis. If you suspect infection, tumor, or bony abnormalities, obtain an MRI or CT scan. MRI has surpassed bone scanning as the gold standard for diagnosing spinal infections, because it confirms a specific anatomic diagnosis. Spondylolysis and spondylolisthesis are 2 of the most common causes of back pain in adolescents; the diagnosis is made with plain radiographs, which show slippage on the later-al view in patients with spondylolisthesis and fracture through the pars interarticularis on the oblique views in those with spondylolysis.
ABSTRACT: Patients can greatly reduce the risk of traveler's diarrhea by drinking only bottled water and eating only hot foods prepared in sanitary conditions or peelable fruits and vegetables. Antibiotic prophylaxis for traveler's diarrhea is no longer routinely recommended; reserve it for patients who may have to consume food and beverages of questionable safety, those with reduced immunity, and those likely to experience serious consequences of illness. Adequate hydration is the first step in treating traveler's diarrhea. Drug therapy-loperamide or fluoroquinolones in adults and bismuth subsalicylate or azithromycin in children-can ameliorate symptoms and speed recovery. Recommend that patients who are prone to motion sickness take an antiemetic/antivertigo agent before symptoms begin. Acetazolamide can be used both to prevent and to treat altitude sickness. Contraindications to air travel include a resting oxygen saturation of less than 90%, pregnancy of more than 36 weeks' duration, pneumothorax, recent myocardial infarction or chest or abdominal surgery, active infectious diseases, and poorly controlled seizures or sickle cell anemia.
ABSTRACT: A thorough history and physical examination can establish the diagnosis of tension headache; further evaluation is generally unnecessary. In contrast, the workup of cervicogenic headache includes standard radiographs, 3-dimensional CT, MRI, and possibly electromyography; nerve blocks may also be used to confirm the diagnosis. Episodic tension headache can be treated effectively by trigger avoidance, behavioral modalities, and structured use of analgesics. Reserve opioids for patients with intractable headaches. Chronic tension headache is treated primarily by prophylactic measures, such as antidepressants and anticonvulsants, and behavioral and physical therapy. Treatment options for cervicogenic headache include analgesics; invasive procedures, such as trigger point injections, greater or lesser occipital nerve blocks, facet joint blocks, segmental nerve root blocks, and diskography; spinal manipulation; and behavioral approaches.
Persistent pain is common in older adults but tends to be underrecognized and undertreated. Up to 50% of community-dwelling older persons have significant painand up to 80% of nursing home residents have substantial pain that is undertreated.
Advertisement
Advertisement
Trending on Patient Care Online
1
Semaglutide Boosts Quality of Life in T2D and CKD, FLOW Trial Analysis Finds
2
5 FDA Decisions for Primary Care to Know from May 2026
3
FDA Issues Complete Response Letter for Cingulate ADHD Drug CTx-1301
4
Practical Strategies for Managing VMS and Cardiovascular Risk in Primary Care
5