


























































































































































A 51-year-old man with a 20-year history of asthma and seasonal allergies presented with low-grade fever, progressive dyspnea on exertion, and wheezing that had persisted for 2 weeks. Four days earlier, he had been seen by his primary care physician and had started levofloxacin therapy. However, his respiratory symptoms had worsened, warranting hospitalization. He also reported pain in the abdomen and left flank and pain and swelling in the right metacarpophalangeal and right shoulder joints.
Asthma
Latest News
Advertisement
Advertisement
As the incidence of asthma continues to increase worldwide, current studies have indicated that the most prevalent challenge to the alleviation of asthma symptoms is undertreatment. Results of a controlled study in Denmark suggest that a physician-managed Internet-based asthma monitoring system can help patients optimize control over their asthma.
Abstract: The standard therapies for acute exacerbations of chronic obstructive pulmonary disease include short-acting bronchodilators, supplemental oxygen, and systemic corticosteroids. For most patients, an oxygen saturation goal of 90% or greater is appropriate. Bilevel positive airway pressure (BiPAP) is usually beneficial in patients with progressive respiratory acidosis, impending respiratory failure, or markedly increased work of breathing. However, BiPAP should not be used in patients with respiratory failure associated with severe pneumonia, acute respiratory distress syndrome, or sepsis. Systemic corticosteroids are appropriate for moderate to severe acute exacerbations; many experts recommend relatively low doses of prednisone (30 to 40 mg) for 7 to 14 days. Antibiotic therapy is controversial, but evidence supports the use of antibiotics in patients who have at least 2 of the following symptoms: increased dyspnea, increased sputum production, and sputum purulence. (J Respir Dis. 2005;26(8):335-341)

A 62-year-old woman with a 25-year history of dyspnea was hospitalized because of hypoxemia. The dyspnea had become more severe during the past few years; it was worse in the standing position, was not exacerbated by walking, and was immediately relieved on lying down. She had no seasonal variation or environmental trigger of the dyspnea.
Abstract: All children with asthma should have periodic office visits, usually every 3 to 6 months, in which asthma action plans are updated. Periodic assessment of lung function by peak expiratory flow or office spirometry can help determine the appropriate treatment strategy. Low daily doses of inhaled corticosteroids remain the first and most effective choice of therapy for persistent asthma. If this approach is inadequate, adding a second medication, such as a leukotriene modifier or a long-acting ß2-agonist, is suggested. Short-acting ß2-agonists remain the most important therapy for intermittent asthma. For most children, the best route is via a metered-dose inhaler with either a spacer or valved holding chamber. If these agents are inadequate, a short course of oral corticosteroids may be required. (J Respir Dis. 2005;26(8):348-358)
How can repeated visits to the emergency department (ED) for asthma exacerbations best be avoided?
Abstract: The classic presentation of anaphylaxis includes urticaria, angioedema, dyspnea, and systemic hypoperfusion. However, anaphylaxis may be more difficult to recognize if syncope, bronchospasm, or cardiovascular collapse is the predominant feature. Essential components of the history include previous allergic reactions, medication use, recently ingested foods, and exposure to latex. Although angioedema is often obvious, it also can be subtle and may require asking patients about changes they have observed. Other findings include tachypnea; wheezing; inspiratory stridor; conjunctival injection; rhinorrhea; and hoarseness, which may suggest laryngeal edema. Oxygen with ventilatory support, epinephrine, and crystalloid volume resuscitation are the mainstays of therapy for anaphylactic shock. Additional therapy often includes H1 antagonists, H2 antagonists, and corticosteroids. (J Respir Dis. 2005;26(7):308-316)
Abstract: Although smoking cessation is still the most impor- tant intervention in chronic obstructive pulmonary disease (COPD), a variety of pharmacologic therapies are available to help manage symptoms. Short-acting ß2-agonists and/or ipratropium should be taken as needed, and the use of additional therapies is based on the severity of disease. Patients with moderate or severe COPD should regularly take 1 or more long-acting bronchodilators. The long-acting ß2-agonists salmeterol and formoterol have been demonstrated to improve health-related quality of life. Newer therapies include the long-acting anticholinergic tiotropium and a salmeterol-fluticasone combination. These agents improve forced expiratory volume in 1 second and may reduce the rate of acute exacerbations. For patients with moderate to very severe COPD, participation in a pulmonary rehabilitation program can improve health status, quality of life, and exercise tolerance. (J Respir Dis. 2005;26(7):284-289)
Stories about community-associated infections with methicillin-resistant Staphylococcus aureus (MRSA) have been making headlines in recent months in both the medical and popular press. A familiar problem in hospitals and nursing homes for decades, growing numbers of MRSA infections have been documented over the past few years in prison inmates, soldiers, athletes, Pacific Islanders, Alaska Natives, Native Americans, and men who have sex with men.
Abstract: Although excessive daytime sleepiness is most often simply the result of inadequate sleep, other causes must be considered as well. Common causes of daytime sleepiness include obstructive sleep apnea/hypopnea syndrome (OSAHS) and medication side effects. The differential diagnosis also includes narcolepsy and restless legs syndrome (RLS). In many cases, the answers to a few simple questions can provide the necessary clues to the diagnosis. Loud snoring is associated with OSAHS, while sudden muscle weakness triggered by intense emotion is consistent with narcolepsy. Referral for sleep evaluation is indicated to evaluate for OSAHS, narcolepsy, RLS, and idiopathic hypersomnia. Methods of measuring daytime sleepiness include the Multiple Sleep Latency Test and the Epworth Sleepiness Scale. (J Respir Dis. 2005;26(6):253-259)
Abstract: ß-Agonists, administered by metered-dose inhaleror nebulizer, are still the mainstay of therapy for asthma exacerbations.A trial of a subcutaneous ß-agonist should beconsidered in patients who fail to respond to inhaled medications.Levalbuterol may play a role in managing refractoryasthma, particularly in patients with ischemic heart disease orsevere tachycardia. Systemic corticosteroids should be administeredto all patients presenting to the hospital withasthma unless their peak expiratory flow rate (PEFR) orforced expiratory volume in 1 second (FEV1) is at least 80% ofpredicted after 1 hour of treatment; this therapy should be institutedwithin 1 hour of presentation. For patients with severeobstruction, the combined use of an anticholinergic and aß-agonist improves PEFR and FEV1 more than ß-agonistsalone and significantly decreases the risk of hospital admission.(J Respir Dis. 2005;26(6):238-249)
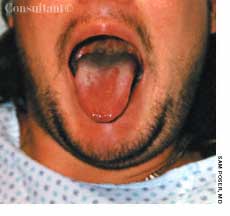
This 41-year-old woman rushed to the emergency department with a swollen, blistered tongue and difficultly in swallowing and speaking. Twenty minutes earlier she had eaten fish (for the first time in her life).
Abstract: High-resolution CT (HRCT) can play an important role in the assessment of bronchiolitis. Direct signs of bronchiolitis include centrilobular nodules, bronchial wall thickening, and bronchiolectasis. Indirect signs include mosaic perfusion, hyperlucency, mosaic or diffuse airtrapping, vascular attenuation, and increased lung volumes. Expiratory HRCT scans are considered an essential part of the workup, because airtrapping may be evident only on these scans. In infectious cellular bronchiolitis, the centrilobular nodules typically have a branching, or "tree-in-bud," appearance, whereas in hypersensitivity pneumonitis, these nodules have a round or nonbranching pattern. The HRCT signs of constrictive bronchiolitis include mosaic perfusion, mosaic airtrapping, vascular attenuation, bronchiolectasis, and bronchiectasis; centrilobular nodules are usually absent. (J Respir Dis. 2005; 26(5):222-228)
Abstract: In most patients, a life-threatening exacerbation of asthma is preceded by a gradual worsening of symptoms. However, some patients have a sudden onset of worsening symptoms, and these patients are at increased risk for respiratory failure and death. Risk factors for near-fatal asthma include a history of a life-threatening exacerbation, hospitalization for asthma within the past year, delay in time to evaluation after the onset of symptoms, and a history of psychosocial problems. Regularly monitoring peak expiratory flow rate (PEFR) is particularly important because it can identify a subset of high-risk patients--specifically, those with large fluctuations in PEFR and those who have severe obstruction but minimal symptoms. Signs of life-threatening asthma include inability to lie supine, difficulty in speaking in full sentences, diaphoresis, sternocleidomastoid muscle retraction, tachycardia, and tachypnea. (J Respir Dis. 2005;26(5):201-207)
The prevalence of asthma in the United States is estimated to be 5% to 8%. Asthma is responsible for approximately 5000 deaths annually in this country. It is a leading cause of emergency department visits, hospitalizations, and school and work absenteeism. The total estimated direct cost of the disease in the United States was $12.7 billion in 1998.
Selective cyclooxygenase-2 (COX-2) inhibitors, such as celecoxib, rofecoxib, and valdecoxib, are an effective and commonly used class of drugs for the management of pain. They are particularly useful in patients who are unable to tolerate aspirin or traditional NSAIDs because of side effects.
Abstract: For some patients with allergic rhinitis, symptoms can be reduced substantially by the use of allergen avoidance measures. However, many patients require pharmacotherapy, including antihistamines, decongestants, and intranasal corticosteroids, to adequately control their symptoms. The oral antihistamines are effective in reducing rhinorrhea, itching, and sneezing but are not effective against nasal congestion. Intranasal azelastine has been shown to be beneficial in patients with moderate to severe symptoms that are not sufficiently controlled by an oral antihistamine. Additional therapies include intranasal ipratropium, which specifically targets rhinorrhea, and cromolyn, which can reduce many of the symptoms of allergic rhinitis and can be used prophylactically. (J Respir Dis. 2005;26(4):150-162)
A study in Finland confirms that many adults with asthma have gastroesophageal reflux disease (GERD) and that many of these persons do not have the classic GERD symptoms. However, the role of GERD as an asthma trigger has not been clearly defined.
ABSTRACT: Education can help improve compliance with inhaled corticosteroid therapy or correct faulty metered-dose inhaler (MDI) technique. Options for patients with poor MDI technique include use of a spacer or an alternative device, such as a nebulizer or a dry powder inhaler. If therapy is ineffective, consider alternative conditions that mimic asthma, especially vocal cord dysfunction and upper airway obstruction. Treatment of comorbid conditions, such as gastroesophageal reflux disease or rhinosinusitis, may improve control. In refractory asthma, it is crucial to identify allergic triggers and reduce exposure to allergens. If another medication needs to be added to the inhaled corticosteroid, consider a long- acting b-agonist, leukotriene modifier, or the recombinant monoclonal anti-IgE antibody omalizumab.
ABSTRACT: The rate at which acute dyspnea develops can point to its cause. A sudden onset strongly suggests pneumothorax (especially in a young, otherwise healthy patient) or pulmonary embolism (particularly in an immobilized patient). More gradual development of breathlessness indicates pulmonary infection, asthma, pulmonary edema, or neurologic or muscular disease. A chest film best identifies the cause of acute dyspnea; it can reveal pneumothorax, infiltrates, and edema. Pulmonary embolism is suggested by a sudden exacerbation of dyspnea, increased ventilation, and a drop in PaCO2. A normal chest radiograph reinforces the diagnosis of pulmonary embolism, which can frequently be confirmed by a spiral CT scan of the chest. Pneumonia can be difficult to distinguish from pulmonary edema. In this setting, bronchoalveolar lavage and identification of the infectious organism may be necessary to differentiate between the 2 disorders.

A 43-year-old woman presented to the emergency department with a 4-day history of worsening erythema, swelling, and pruritus that developed on the face and progressed to the abdomen, back, and lower legs. In the past 2 to 3 days, fluid-filled blisters had arisen, followed by skin sloughing; the patient also reported subjective fevers. Another physician had prescribed naproxen for back pain 6 days earlier. The patient had a history of asthma, with rare inhaler use, and depression, for which she had taken citalopram for 2 years.
Several new drugs are being introduced-and more are on thehorizon.
A 48-year-old woman with a historyof hypertension and mildasthma has been transferred to themedical service because of an abnormalpostoperative ECG. She hadbeen admitted 2 weeks earlier to thegynecology-oncology service for localrecurrence of a previously resecteduterine sarcoma and underwent laparotomyfor debulking of the pelvicmass and resection of the rectosigmoidcolon. She did well until postoperativeday 14, when sudden chestpain and dyspnea developed.
Because bariatric surgery has traditionally been associated with a high incidence of complications, it has been used primarily for superobese patients. A large body of evidence suggests that laparoscopic adjustable gastric banding is a much safer procedure that is also very effective. This procedure offers an additional option to patients who might benefit from bariatric surgery when diet, exercise, and pharmacologic approaches have failed. Here we address questions primary care physicians often ask about the procedure.
Most sport-diving problems are mild and self-limited; however, serious or life-threatening situations can arise. In a previous article (CONSULTANT, June 2004, page 961), we addressed fitness and safety issues. In this article, we review the principal medical problems associated with sport diving.
Advertisement
Advertisement
Trending on Patient Care Online
1
Early Liver Disease Detection Starts in Primary Care: A Q&A With Stevan Gonzalez, MD
2
Retatrutide Achieved Up to 22.6% Weight Loss in 2 Phase 3 Obesity Trials
3
Compulsive Smartphone Use Linked to Depressive Symptoms in Older Adults
4
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
5