



















































































































































































































The use of analgesics, specifically acetaminophen, has been proposed as one of the mechanisms for the rise in asthma prevalence in the last 30 to 40 years.1 Acetaminophen, approved by the FDA in 1951, is one of the most commonly used analgesics in adults and children. The association between asthma and acetaminophen has been reported in case reports, in the setting of oral challenge tests, and in larger clinical studies.2
Asthma
Latest News
Advertisement
Advertisement
A 24-year-old Korean woman, who was 20 weeks' pregnant, was referred to an allergist for an elimination diet and evaluation of the risk of allergies to her unborn child. She had a several-year history of perennial allergic rhinitis with seasonal exacerbations.
Abstract: Chronic rhinosinusitis can be caused or aggravated by a number of factors, including bacterial, viral, and fungal infections; asthma; allergies; and obstruction caused by nasal polyps or a deviated nasal septum. The diagnosis can usually be established clinically. Imaging studies are not routinely necessary, but a CT scan of the sinuses should be obtained if the patient has significant ocular or orbital symptoms or if sinus surgery is planned. Treatment consists of antibiotics, with consideration of a change in the regimen if the patient has already received a full course of a first-line agent. The course of treatment may need to extend to 4 weeks. Also consider adjunctive therapy, such as intranasal corticosteroids and decongestants. Patients who have allergic rhinitis may also benefit from an antihistamine and/or a leukotriene modifier. Sinus surgery is reserved for patients who do not respond to medical therapy. (J Respir Dis. 2005;26(10):415-422)
A 4-year-old boy is admitted with a 2-week history of high fever with rigors; profuse night sweats; progressive dull, aching, nonradiating right upper quadrant pain; and watery, foul-smelling diarrhea that contains no blood or mucus.
In patients with underlying disease, a preoperative evaluation and targeted perioperative management strategies can minimize surgical complications and maximize healing. This article focuses on how to identify surgery patients at risk for complications caused by diabetes, chronic obstructive pulmonary disease (COPD), and other medical conditions; I also describe strategies to minimize such risk.
A 14-year-old African American boy presented during the winter months with a painless, nonpruritic, periumbilical rash that had been present for approximately 1 month. Initially bluish, the rash had become dark brown.
Under what circumstances would asthma or chronic obstructive pulmonary disease (COPD) be a contraindication to scuba diving? What precautions should patients with either asthma or COPD take if they are determined to go diving?
Abstract: Although controller therapies are currently recommended for patients who have persistent asthma, a number of studies indicate that these therapies do not adequately control asthma in a substantial number of these patients. This observation, combined with the potential risk of adverse effects with corticosteroids, supports the conclusion that controller therapies are not appropriate for all patients. However, some patients who do not respond to one type of controller therapy will respond to another, which suggests that we might consider targeting specific medications to select patients. There is increasing evidence that certain biomarkers may be useful in guiding therapy. For example, levels of sputum eosinophils have been shown to predict which patients are at increased risk for deterioration of asthma when inhaled corticosteroids are withdrawn.
Abstract: There is convincing evidence that controller therapies, such as inhaled corticosteroids and leukotriene receptor antagonists, provide many benefits to patients with asthma. These benefits include decreased symptoms, improved lung function, reduced frequency of exacerbations, and improved quality of life. Even patients with mild asthma and normal lung function can benefit from controller therapy. A recent analysis of the burden of asthma suggests that the proportion of patients who have mild intermittent disease is much smaller than previously estimated and that many more patients have persistent asthma. This finding, in combination with the considerable variability of patient responses to therapy and the difficulty in predicting which patients will respond, underscores the importance of considering a trial of controller therapy in patients with asthma.
Abstract: Pulmonary function tests, such as the measurement of forced expiratory volume in 1 second (FEV1) and peak expiratory flow (PEF), provide an objective, standardized, and quantifiable method of patient assessment and can be essential in the evaluation of asthma. However, FEV1 and PEF are relatively insensitive for detecting changes in persons with good baseline pulmonary function, and they do not directly measure worsening airway inflammation. One way to deal with the shortcomings of these tests is to include multiple outcomes assessment. Evaluating patient-oriented variables, such as symptoms, need for rescue medication, nocturnal awakenings, and unscheduled medical care visits, can detect clinically relevant changes that pulmonary function tests do not identify. Composite outcomes provide a more comprehensive approach to patient follow-up. For example, a patient who is considered to be a "nonresponder" to a given therapy on the basis of pulmonary function criteria might, in fact, be responding favorably according to assessment of composite outcomes. Two patient-centric tools for measuring outcome are the asthma control questionnaire and the asthma control test.
Asthma is one of the most common chronic diseases worldwide, and its prevalence--particularly among children--is increasing in many countries.1,2 In 1997, an estimated 9.6% of persons in the United States had asthma (Table 1).3
Dr Storms: Given that a patient's asthma varies quite a bit from day to day, and that controller therapies can prevent exacerbations, is there any role for using a controller medication as-needed rather than using it regularly? Could exacerbations be prevented if the patient has been educated to start treatment as soon as symptoms occur or peak expiratory flow (PEF) falls?
Abstract: The coexistence of asthma and obstructive sleep apnea (OSA) in a given patient presents a number of diagnostic and treatment challenges. Although the relationship between these 2 diseases is complex, it is clear that risk factors such as obesity, rhinosinusitis, and gastroesophageal reflux disease (GERD) can complicate both asthma and OSA. In the evaluation of a patient with poorly controlled asthma, it is important to consider the possibility of OSA. The most obvious clues are daytime sleepiness and snoring, but the definitive diagnosis is made by polysomnography. Management of OSA may include weight loss and continuous positive airway pressure (CPAP). Surgical intervention, such as uvulopalatopharyngoplasty, may be an option for patients who cannot tolerate CPAP. Management may include specific therapies directed at GERD or upper airway disease as well as modification of the patient's asthma regimen. (J Respir Dis. 2005;26(10):423-435)

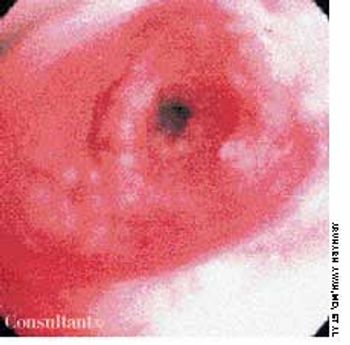
A 69-year-old woman was admitted to the hospital with wheezing and dyspnea. She also complained of hoarseness and slight dysphagia that had caused a loss of 12 lb during the past 4 months. The patient had been treated for bronchial asthma as an outpatient, but the worsening episodes of wheezing were not being controlled by bronchodilator therapy.

The 83-year-old woman whose hands are shown in photograph A had a severe flare of arthritis in the metacarpophalangeal and proximal interphalangeal (PIP) joints after corticosteroid therapy for her asthma was stopped. The clue to the diagnosis of psoriatic arthritis is in her fingernails, which show both pitting and onycholysis.

A 37-year-old woman presented with progressive dyspnea of 2 weeks' duration, a low-grade fever, and night sweats. She had been a healthy marathon runner until her exercise tolerance recently declined.
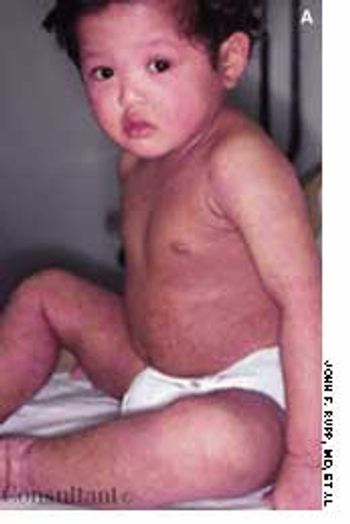
The onset of atopic dermatitis can be seen in infants who have a family history of inhalant allergies, (eg, seasonal allergy, allergic rhinitis, or allergy-induced asthma). The cheeks and large flexural folds of affected children are erythematous and scaly. Involved areas of the trunk and extremities may exhibit discrete patches or a generalized rash.

A chest roentgenogram from a 42-year-old man with asthma, primary hypoparathyroidism, and pectus excavatum showed a left suprahilar mass-like density.

This rash, which covered a 68-year-old woman's body, was noted to have worsened during the past 2 months. A cephalosporin antibiotic had failed to clear the condition. The patient, a nursing home resident, suffered from emphysema, asthma, and heart disease. She had been receiving oxygen therapy and prednisone for 1 year.

A 12-year-old boy with a history of atopy complained of pruritus and severe dryness of the hands. Over-the-counter moisturizers failed to resolve the condition. The patient did not wash his hands frequently and had no hobbies that exposed him to environmental irritants or allergens.
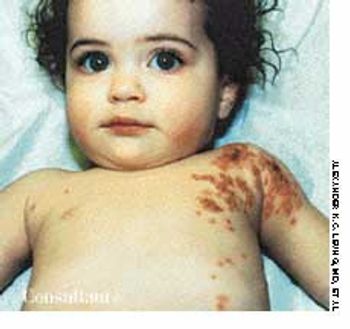
Five days before this 1-year-old girl was brought to her doctor's office, a rash had developed on her left shoulder and the left side of her chest. The abrupt onset of a high fever (temperature, 41°C [105.8°F]) and irritability accompanied the outbreak of the rash. The child had a history of asthma and eczema.
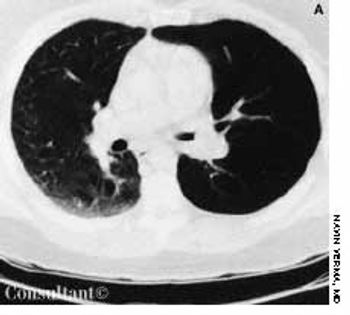
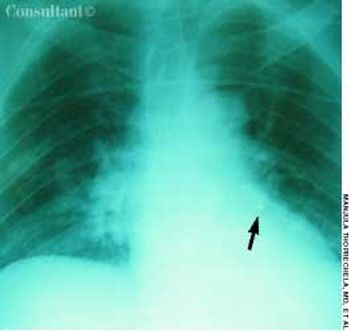
With a 1-year history of episodic wheezing, a 62-year-old woman (a smoker for the past 30 years) was being treated for bronchial asthma, but bronchodilator therapy did not control her symptoms. She was hospitalized with worsening dyspnea and a 4.5-kg (10-lb) weight loss over the past 3 months. There was no hemoptysis.
A 40-year-old man was being treated as an outpatient with inhaled corticosteroids and bronchodilators for a presumed diagnosis of bronchial asthma. Worsening episodes of shortness of breath during the past few months sent him to the emergency department for a second opinion.
For 1 month, an 82-year-old woman had had episodes of coughing. Chronic bronchitis had been diagnosed; however, antibiotics and bronchodilators failed to control symptoms.
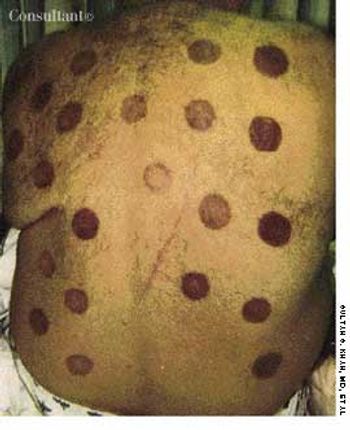
An acute exacerbation of asthma brought this 52-year-old Russian emigré to the emergency department (ED). Examination revealed the well-demarcated round erythema and ecchymosis on the patient's back. This circular pattern was created by cupping performed 2 days earlier by the patient's wife in an effort to treat her husband's asthma.
Advertisement
Advertisement
Trending on Patient Care Online
1
Nearly 18 Million Middle-Aged US Women Overdue for Cancer Screening, Study Finds
2
When CPAP Fails: Expert Discussion on How to Counsel Patients With OSA
3
OSA Treatment Beyond CPAP: Tirzepatide, Phenotyping, and What's Next, With Ashesha Mechineni, MD
4
Tirzepatide and Emerging OSA Pharmacotherapy Expand the Treatment Toolkit, With Ashesha Mechineni, MD
5