Articles by Andrew L. Wong, MD

This obstruction is caused by a failure of intestinal peristalsis; there is no evidence of mechanical obstruction. Paralytic ileus is common after abdominal surgery, especially if anticholinergic drugs are given preoperatively and/or narcotics are used postoperatively. It usually lasts 2 to 3 days. Paralytic ileus may also be caused by peritonitis; ischemia or surgical manipulation of the bowel; retroperitoneal hemorrhage; spinal fracture; systemic sepsis; shock; hypokalemia; uremia; pharmacologic agents (eg, vincristine, loperamide, and calcium channel blockers); diabetic ketoacidosis; and myxedema.

A 3-month-old female infant presented with a mass in the umbilical area. During the neonatal period, an infection of the umbilical cord had resulted in the formation of exuberant granulation tissue at the base of the umbilicus.

This condition involves the invagination of a proximal segment of bowel (the intussusceptum) into a more distal segment (the intussuscipiens). It occurs most frequently in infants between the ages of 5 and 12 months and is a leading cause of intestinal obstruction in children aged 2 months to 5 years. Intrauterine intussusception is associated with the development of intestinal atresia. The male to female ratio is approximately 3:2. Intussusception is slightly more common in white than in black children and is often seen in children with cystic fibrosis.

A 2-year-old girl presented with a 2-day history of urinary frequency and dysuria. Physical examination revealed complete fusion of the labia minora. Urine culture showed Escherichia coli with a colony count of 108/L. The child was treated with a 10-day course of amoxicillin that resulted in complete clearance of the urinary tract infection.

This disorder occurs in fetal development, when the midgut supplied by the superior mesenteric artery grows too rapidly to be accommodated in the abdominal cavity. Prolapse into the umbilical cord occurs around the sixth week of gestation. Between the tenth and eleventh weeks, the midgut retracts from its location at the exocelomic umbilical stalk back into the abdominal cavity. During this return, the midgut undergoes a 270-degree counterclockwise rotation about the axis of the superior mesenteric artery, followed by fixation to the posterior abdominal wall. Malrotation results from failure of the midgut to properly rotate and affix itself to this wall. This disorder occurs approximately once in 500 live births.

A 12-year-old boy was brought to his physician because of a tensely cystic mass in the right side of the scrotum. The spermatic cord could be felt above and below the lump. It had no cough impulse.
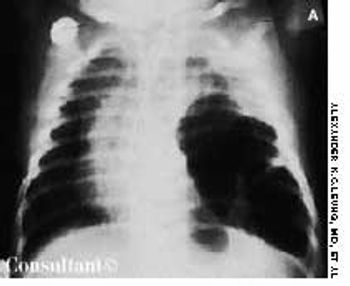
An irritable, lethargic, toxic-looking, and slightly cyanotic 2-month-old boy had a temperature of 40°C (104°F), malaise, and a cough for 2 days. The infant's heart rate was 98 beats per minute, and his respiratory rate was 55 breaths per minute. He had nasal flaring, sternal and subcostal retractions, diminished breath sounds, and scattered rales over the left lung, which was dull to percussion.

A 10-year-old boy presented with a 6-month history of a painless mass on the left side of the scrotum. The overlying skin had a bluish discoloration. The mass felt like a “bag of worms.” When the boy stood, venous varicosity could be palpated along the spermatic cord. This venous distention increased when he performed Valsalva's maneuver and decreased when he was recumbent.

Severe pain in the scrotum during a soccer game sent a 14-year-old boy to his physician. The right testicle was swollen and exquisitely tender. On exploration, it was hemorrhagic and blue-black. A small incision in the tunica of the testis revealed arterial bleeding, which indicated that the testis was still viable. The right testicle was untwisted and fixed to the scrotum.

A 37-year-old man presented with a reddish nodule in the umbilical area that had been present since early infancy. The lesion had been cauterized with silver nitrate several times in the past but had not resolved. No drainage or secondary infection was noted, and the patient was otherwise in good health.

Also known as congenital aganglionic megacolon, this condition is characterized by a congenital absence of ganglion cells in the submucosal (Meissner) plexus and the myenteric (Auerbach) plexus in one or more segments of the colon. This is attributable to a failure of migration of nerve cell elements from the neural crest in a cephalocaudal direction along the GI tract. The absence of parasympathetic innervation causes failure of relaxation of the internal anal sphincter. An aganglionic colon does not permit normal peristalsis to occur and thus results in a functional obstruction.

An infant born to a 25-year-old gravida 2 para 1 mother by cesarean section at 36 weeks' gestation had loops of small intestine protruding from the abdominal cavity.

The parents of a 3-month-old infant sought medical advice because of a mass in the child's umbilical area. The mass increased in size when the infant cried, coughed, or strained and was reducible inside the abdomen by external pressure.

A 6-year-old boy presented with a mass on the left side of the scrotum. The mass did not vary in size and was asymptomatic; it transilluminated brightly. Physical examination showed it to be 4 × 2 cm. The spermatic cord could be felt above the mass. The left testis was impalpable separately.

The mother of a 2-year-old boy was concerned because his scrotum appeared flat and empty. (She had noticed this earlier but thought it was normal for her child's age.) On examination, the testicles were not palpable in the scrotum. They were found in the inguinal area and could not be manipulated into the scrotum. Bilateral orchidopexy was performed, and the postoperative course was uneventful.

The extent of mucosal or transmural intestinal necrosis varies. Pneumatosis progresses from the submucosa through the muscular layer to the subserosa. The distal ileum and proximal colon are most frequently involved.

Inspissated, sticky, immobile meconium causes this transient form of distal colonic or rectal obstruction in newborns. The incidence has been estimated at 1 in 500 to 1000 live births. The condition is thought to result from dehydration of the meconium.

A mass on the left side of the scrotum was the presenting complaint of a 7-year-old boy. The mass increased in size when the child cried, strained or coughed. Physical examination showed a left scrotal mass that was reducible with manipulation when the child was lying down. The left spermatic cord was found to be thickened-the "silk" sign.

This obstruction results from hypertrophy of the circular and longitudinal muscularis of the pylorus and the distal antrum of the stomach. It occurs in approximately 3 of every 1000 live births and is 4 times more common in boys. Pyloric stenosis (PS) is relatively uncommon in African American and Asian infants. The observation that it occurs primarily in first-born infants has been disputed.

A mass covered by a translucent membrane was found in the umbilical area of an infant born by cesarean section at 38 weeks' gestation to a 26-year-old gravida 3 para 2 mother.

This condition is characterized by a localized narrowing of the jejunum without a disruption of continuity or defect in the mesentery. At the stenotic site, there is often a short, narrow segment with a minute lumen where the muscularis is irregular and the submucosa is thickened. The resultant intestinal obstruction is incomplete.

Congenital adrenal hyperplasia is an autosomal recessive disorder. Deficiency of 21-hydroxylase accounts for 95% of all cases.

A painful, swollen penis was the presenting complaint of an 11-year-old boy. The swelling erupted 1 to 2 hours before the photograph was taken, when the child had attempted to retract the foreskin.

Affected infants present shortly after birth with a large bowel obstruction secondary to transient dysmotility in the descending colon. Although the cause is unknown, immaturity of the colonic myenteric plexuses has been demonstrated in some cases. More than 50% of affected infants are born to mothers with diabetes. Other predisposing factors include hypoglycemia and sepsis.

This condition, which accounts for about 30% of cases of intestinal obstruction among neonates, is characterized by the inspissation of thick, tenacious meconium in the bowel. The most common cause is cystic fibrosis; approximately 6% to 20% of infants with cystic fibrosis have meconium ileus. Hyperviscous mucus secreted by abnormal intestinal glands, an abnormal concentrating process in the proximal small intestine, and a deficiency of pancreatic enzymes have been implicated in the pathogenesis. The histologic hallmark is distention of the goblet cells in the intestinal mucosa.

A 7-year-old boy presented with two testicles on the left side of the scrotum. The superior one was half the size of the inferior one, which measured 2 × 1 cm. The testicle on the right side measured 2 × 1 cm. Surgical exploration was done, and the atrophic left supernumerary testicle shown in the photo was removed. Biopsy specimens taken from the remaining testicle were normal.
Alimentary tract duplications are uncommon. Gastric duplication accounts for only 3.8% of these duplications. The cause is not known, but faulty separation of the endoderm and notochord early in embryonal development is thought to be responsible. The anomaly occurs in twice as many female as male infants.

A female infant was born vaginally to a gravida 4, para 1, 24-year-old woman at term. The child's birth weight was 2,800 g; her length was 51 cm. The mother had a history of three spontaneous abortions. The present pregnancy was complicated by threatened abortion at 15 weeks. The mother was given hydroxyprogesterone hexanoate, 500 mg IM weekly for 6 weeks.

During the last few weeks of gestation or shortly after birth, the layers of the processus vaginalis normally fuse together and obliterate the entrance to the inguinal canal in the vicinity of the internal inguinal ring. An indirect hernia results from a failure of fusion of the processus vaginalis; the bowel subsequently descends through the inguinal canal.

The mother of a 1-month-old infant was concerned because her child's umbilicus looked abnormal. The condition was diagnosed as umbilicus cutis.






