
























































































































































Brain cell damage similar to that seen in Alzheimer disease and other disorders results when a gene that controls the sleep-wake cycle and other bodily rhythms is disabled.
Neurology
Latest News

Advertisement
Advertisement
Daily acute intermittent hypoxia and dAIH combined with overground walking improved walking speed and distance in persons with chronic incomplete spinal cord injury.
Women who have post-traumatic stress disorder gain weight more rapidly than women who do not and are more likely to be overweight or obese.

Do you know what the ACIP says about mixing the zoster and varicella vaccines?
Four inpatient detentions in 4 months, but Jennifer happily caught a bus to head home. Was this case another crisis averted? Or just another flagrant waste of limited funds?
This just in: Medicare reimburses physicians 3 to 5 times more for common procedural care than for cognitive care.
Lowering blood sugar levels is a promising strategy for preventing memory problems and cognitive decline as persons age, even for those whose blood sugar levels fall within the normal range.
Electric stimulation of peripheral nerves shows promise as a long-term treatment for patients with chronic headache.

Peanut butter and a ruler may turn out to be tools that offer an inexpensive, sensitive, and specific olfactory means of screening for Alzheimer disease. Details here.
Neurological disorders have been considered a significant threat to public health for some time. Take a look at these facts and figures.
In its classic form, ALS affects motor neurons at 2 or more levels supplying multiple regions of the body.
Charles Bonnet syndrome is an uncommon condition causing visual hallucination in patients who do not have mental illness
The drive to screen older persons for minor memory changes is leading to unnecessary investigation and potentially harmful treatment, according to some experts.
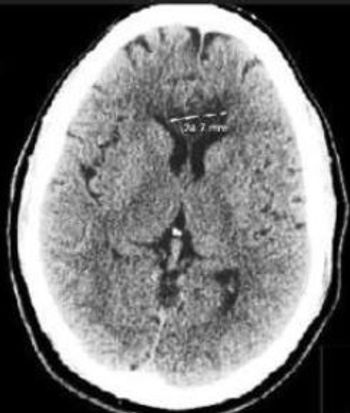
Bilateral strokes of the corpus callosum are uncommon because of the rich blood supply of this structure from three main arterial systems.

Skin eruptions, MS risk, and a pain in the back: 5 new questions-your Dxs?
As biomarkers to detect signals of Alzheimer disease improve at providing clinically meaningful information, a majority of Alzheimer researchers support disclosing results to research subjects who have these tests.
Urinary protein levels may be an early marker of future cognitive decline in patients with type 2 DM and normal kidney function, according to a new study.
A gene variant strongly associated with development of type 2 diabetes mellitus appears to respond to a Mediterranean diet to prevent stroke.
Clipping the hardened toenails of a mentally ill patient made me wonder whose hands care for the feet of countless others who can't care for themselves.
The current study may help create new pathways for better understanding and developing more effective and more specific medications.
This agent has a large number of drug-drug and drug-food interactions, and there is a need for increased INR monitoring.
Brain infarcts among crack cocaine users may be secondary to large cerebral artery vasospasm with secondary intravascular thrombosis (with or without distal embolization).
Nonadherence to antihypertensive drug therapy increased risk of stroke, hospitalization for stroke and stroke-related mortality.
The coexistence of focal seizures and secondary generalized seizures in this patient and the respective EEG and MRI findings constitute her peculiar epilepsy syndrome.
One simple addition, basketball, is doing more for health and mental health in this community than months or years of therapy or any number of medications or office visits with me.
Advertisement
Advertisement
Trending on Patient Care Online
1
FDA Approves mRNA-1010 (mFLUSIVA) as First mRNA Flu Vaccine for Adults 50 and Older
2
FDA Reviews Clesrovimab for Second-Season RSV Prevention in High-Risk Children
3
Integrating Social Determinants of Health Into Primary Care: A Team Based Population Health Approach
4
FDA Approves Oveporexton, First Orexin Receptor Agonist for Narcolepsy Type 1
5