


























































































































































Chronic fatigue syndrome (CFS) is a distinct disorder characterized by debilitating and often recurrent fatigue that lasts at least 6 months but more frequently lasts for longer periods. Patients with CFS experience overall physical, social, and mental impairments and may subsequently qualify for medical disability.
Neurology
Latest News

Advertisement
Advertisement
Primary care is demanding for a host of reasons, not the least of which is the daunting breadth of issues practitioners grapple with. One issue is evaluating the risk of suicide. Two recent studies provide some intriguing data that may change the way we practice.

For the past year, a 52-year-old man had dysphagia, which he described as a “knot stuck in the throat” and an associated 25-lb weight loss. He denied fever, chills, headache, abdominal pain, and diarrhea. The patient had been living in the Dominican Republic until about 1 year earlier, when he moved to the United States. He had a 30 pack-year smoking history; he also had hypertension, asthma, and coronary artery disease (none of which were pharmacologically treated). He denied alcohol and illicit drug use.
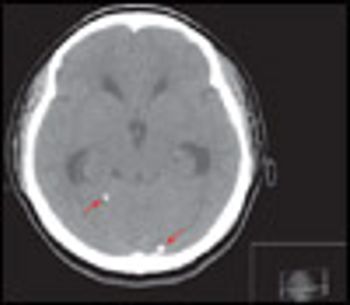
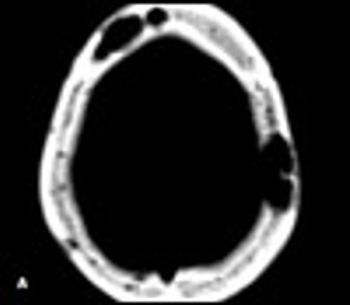
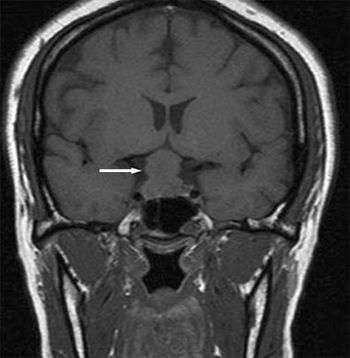
An 18-year-old woman from Mexico was hospitalized because of severe headache with nausea and vomiting. Her headaches had started 4 years earlier and had progressively worsened. They occurred mainly in the occipital region and were pulsating, worse on bending down, and unrelieved by any medication. They were often accompanied by dizziness and presyncope.
After listening to the previous 3 podcasts, you may be wondering how to begin a therapeutically valuable conversation with your patient, which will provide the critical details that you need in the short time that you have. In his final podcast, Dr Lieberman offers a list of questions that you can use to break the ice and kick start a dialog with a patient whom you suspect has a mental health disorder.
It can sometimes be difficult to detect the fine tremors of the hands and fingers of a patient with hyperthyroidism.
A 65-year-old man, who was lost to follow-up after abdominal-perineal resection for rectal adenocarcinoma 9 months earlier, presents with progressively worsening neurological symptoms, including bilateral hearing loss, dizziness, gait disturbance, ataxia, and blindness in the right eye.
A39-year-old man with a history of AIDS and nonadherence to highly active antiretroviral therapy (HAART) presented with frontal headache and scalp pain of 2 weeks' duration. These symptoms were accompanied by nausea, weight loss, and generalized weakness. Physical examination revealed a small, tender scalp lump, 2 × 2 cm over the left parietal area. The findings from the rest of the examination were unremarkable.
Primary care physicians treat the majority of patients in this country who have mental health disorders. But how well prepared are we for these patients when they present to our offices?
In this podcast, Dr Lieberman discusses the associated features of three specific mental disorders: anxiety, major depressive disorder, and bipolar disorder. He offers practical techniques that can be used in diagnosing each of these disorders and provides suggestions for treatment.
Stress affects daily activities, influences the way symptoms are perceived, and detracts from quality of life; it plays a role in everyone’s life and is a component of every illness. The responsibility of the primary care physician is to help manage the stress and recognize when specific therapeutic measures are needed. The fourth edition of The Fifteen Minute Hour presents biopsychosocial approach concepts from the earlier editions of the book and provides new material to make the principles and techniques more useful to primary care health professionals.
Primary care physicians are often the first to see patients with mental health problems and they provide 70% of metal health care to patients. They also write a majority of the prescriptions for antidepressant and antianxiety medications in the United States. This is understandable in light of the fact that physical and mental ailments are often comorbid. But, there may be more to treating a patient who presents with depression than prescribing a pill.
What associated disorders should primary care clinicians be alert for in patients with Parkinson disease?

A 42-year-old woman had a "life-long" history of mild to moderate low back pain, without radiation, anesthesia, weakness, or incontinence. She denied recent trauma or an inciting event. The pain was constant and worse at the end of the day and with prolonged activity. Physical therapy, NSAIDs, tramadol, opioids, and manipulation provided minimal relief.
A 26-year-old woman at 30 weeks’ gestation presented to the emergency department with a throbbing frontal headache of 1 month’s duration. She had also had peripheral blurred vision for the past 2 weeks. Acetaminophen initially decreased her pain but was no longer effective. She had had a previous miscarriage.
Doctors, especially primary care doctors, love stories. We love hearing them from patients and telling them to one another. “Anecdotal learning” it’s called by some (somewhat derisively because it’s not science).

Several days earlier, a 69-year-old man had a mild headache, fatigue, and tingling and prickly facial sensations. Shortly afterward, this painful, “weepy” rash developed on his forehead, upper cheek, and nasolabial folds and vision in the right eye became blurry. The patient’s history included type 2 diabetes mellitus, hypertension, and childhood varicella.
2009 IHC Podcasts
Migraine and chronic daily headache may be risk factors for the development of complex regional pain syndrome, according to the results of a study led by B. Lee Peterlin, DO, assistant professor of neurology, Drexel University College of Medicine in Philadelphia.
Results of a large survey show that many patients with cluster headaches (CH) are not receiving treatment with acute and preventive therapies.
Did Pablo Picasso suffer from migraine? And did these episodes influence his artwork? Not likely, said Joost Haan, MD, PhD, a member of the department of neurology at Leiden University Medical Centre, Leiden, the Netherlands. He discussed migraine and the works of master painters at the 14th annual International Headache Congress in Philadelphia.
Results of a landmark study showed that onabotulinumtoxinA effectively reduced headache symptoms, episodes, disability, and health-related quality of life in patients with chronic migraine.
Patients with migraine accompanied by depression or anxiety disorders had greater improvements in headache-related disability than those without a psychiatric disorder, according to results of the Treatment of Severe Migraine trial.
About 20% of soldiers returning from Iraq and Afghanistan who have a history of concussion or blast exposure experience chronic daily headache, according to a results of study presented at the 14th annual International Headache Congress in Philadelphia.
The portrayal of headache in film may contribute to patients’ misconceptions and fears about their illness, according to Bert B. Vargas, MD, clinical professor of neurology at the Mayo Clinic in Phoenix.
Advertisement
Advertisement
Trending on Patient Care Online
1
FDA Approves SimpleScreen CRC Blood Test for Colorectal Cancer Screening
2
Bepirovirsen and the Push to Close Hepatitis B Care Gaps
3
Noninvasive Testing and the Colorectal Cancer Screening Gap, With Mark Fendrick, MD
4
FDA Grants Fast Track Designation to HTX-001 for Symptomatic Nonobstructive Hypertrophic Cardiomyopathy
5