


























































































































































Medication is seldom necessary. Education is the key element of therapy. An explanation of the process and a discussion of possible triggers-lack of sleep, stress, missed meals etc-is the most key intervention.
Neurology
Latest News
Advertisement
Advertisement
Primary care physicians need to be aware of the relationship, especially because the incidence in older women is high.
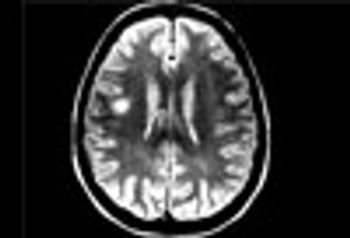
MRI is now central to the diagnosis of multiple sclerosis. Because of the modality’s high sensitivity to inflammation and demyelinating plaques, roughly 90% of all MS diagnoses are now based on MRI findings.
Sodium levels are known to be elevated inside the brain stem, cerebellum, and temporal poles early in the course of MS. This study showed total sodium concentrations to be significantly increased in advanced disease-particularly in normal-appearing brain tissues, concomitant with disability.
After a cardiac event, many patients experience psychiatric symptoms, including depression, but more recent studies have paid attention to anxiety.
Patients who are experiencing pseudoexacerbations or confirmed exacerbations of disease should be assessed and monitored for depressive and anxiety symptoms.
Signs and symptoms of organophosphate poisoning occur through an exaggerated cholinergic or nicotinic response at the neuronal synapse.
The excessive number of deaths in placebo-treated patients largely was the result of MS-related causes, especially MS-related pulmonary infections.

Epstein Barr virus activates potentially immunopathogenic and neuropathogenic proteins in cells deriving from peripheral blood mononuclear cells and astrocytes.
The monoclonal antibody alemtuzumab reduced disease progression and accumulation of disability versus interferon in phase 3 clinical trials.
The overall decreased cancer prevalence in patients with MS warrants further study and may represent an effect of increased immune surveillance in this autoimmune disease.
If physicians know how well their patients tolerate uncertainty about health before providing feedback during a consultation, they can improve their patients' care dramatically.
First-line agents include selective serotonin reuptake inhibitors and venlafaxine.
Many patients clearly would benefit from help from clinicians, but two-thirds of patients have never sought medical care for this disorder.
In this video, Armistead Williams III, MD, of the International Multiple Sclerosis Management Practice in Manhattan, speaks about the primary care physicians’ role in the care of patients with this complex illness.

The patient had been having slurred speech and trouble swallowing and chewing. He had been using his hand to hold his jaw closed and to push his jaw up to help him chew.
Here: more evidence that with the proper tools and motivation, health and wellness are attainable goals-even within the constraints of MS.
Here, Armistead Williams, III, MD, of the International Multiple Sclerosis Management Practice in Manhattan, speaks directly to neurologists about the hard questions that need to be addressed about this complex illness.

What is a safe, effective, and inexpensive way to reduce the risk of heart attacks, strokes, and dementia? What we eat is a key part of the answer. For one thing, doctors can suggest an appropriate diet to motivated patients, or to those who prefer a non-drug approach.
School performance is more likely to be below average in children who have migraine than in those who do not have headaches.
Here: a project that sheds some light on the potential of an integrated and holistic approach to therapy for patients with multiple sclerosis.
What happens when complementary and alternative therapies are combined with traditional treatments in patients with multiple sclerosis? A new study suggests some positive benefits. Details here.
Venous thromboembolism is twice as likely to develop in patients with multiple sclerosis than in controls. Although the absolute risk of VTE is low in MS patients, thromboprophylaxis may need to be considered.
Physical inactivity is more common among patients with multiple sclerosis (MS) than the general public-even though studies have shown that exercise can reduce the frequency and intensity of MS symptoms. Here's a motivational technique that may help.
Meta-analyses of all available data have shown that smoking is associated with a 50% increased risk of MS.
Advertisement
Advertisement
Trending on Patient Care Online
1
FDA Approves mRNA-1010 (mFLUSIVA) as First mRNA Flu Vaccine for Adults 50 and Older
2
FDA Reviews Clesrovimab for Second-Season RSV Prevention in High-Risk Children
3
Integrating Social Determinants of Health Into Primary Care: A Team Based Population Health Approach
4
FDA Approves Oveporexton, First Orexin Receptor Agonist for Narcolepsy Type 1
5