



























































































































































A 35-year-old woman presented to the emergency department (ED) with 2 black eyes, facial swelling, and other injuries (Figure 1). She said that she had been in an all-terrain vehicle accident the day before, in which she hit her face on the handlebar. She said she had lost consciousness for an unknown period and since the accident had experienced headache, dizziness, nausea, and pain over much of her body.
Neurology
Latest News
Advertisement
Advertisement

During a routine physical examination, multiple, randomly distributed, fleshcolored nodules were noted on the trunk, arms, and face of a 62-year-old man. The lesions measured 0.5 to 1.0 cm and appeared slightly pedunculated. The patient had had the lesions since he was a teenager; they were not painful. He also had hypertension, for which he was taking lisinopril (20 mg once daily).
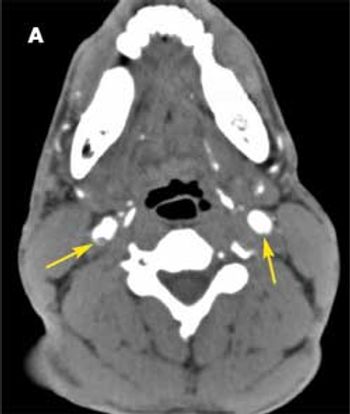
A 37-year-old man was brought to the emergency department (ED) after he had 2 near-syncopal events. The first occurred in the morning and rapidly resolved; the second occurred later in the day at work. The night before he had a headache and neck pain. In the ED, he reported left arm and leg weakness and was noted to have left facial droop.
Losing weight can significantly reduce intracranial pressure and the complications it causes, including headache and optic nerve anomalies.
Most uncomplicated anxiety disorders can be treated in the primary care setting. Following the initial treatment, patients require ongoing care, which combines psychosocial and psychopharmacological therapies. Treatment of anxiety disorders can lead to improved interpersonal, social, and vocational functioning.
Highlights from the International Headache Congress are presented by Stephen D. Silberstein, MD, professor of neurology at Jefferson Medical College and director of the headache center at Thomas Jefferson University, Philadelphia, as well as chair of the congress organizing committee.
Randolph W. Evans, MD, chief of neurology at Park Plaza Hospital and clinical professor at Baylor College of Medicine in Houston, Texas, reviews postconcussion syndrome and post-traumatic headache.
Anxiety disorders are as prevalent and disabling as depression; they affect about 19.1 million adults in the United States at some point during their lifetimes.1-3 Because of the high suicide risk associated with depression, patients who have anxiety may attract less attention from their primary care providers. Thus, anxiety disorders often go undiagnosed and untreated.
A 51-year-old man was hospitalized for subacute alteration of mental status. The patient had a history of alcohol abuse. He had no other medical disorders. Vital signs were normal. The patient scored 15 out of 30 on the Mini-Mental State Examination. He had an ataxic gait; all other physical findings were normal. The family reported that he had been treated in the emergency department 3 days earlier for hypoglycemia. Results of a complete metabolic profile and complete blood cell count were normal.
A 22-year-old man seeks medical attention at his college’s infirmary. He had been in excellent health until 1 week earlier, when he noted onset of fever, headache, and malaise.
The patient has a small-fiber sensory neuropathy that is managed with lamotrigine. She is a physical therapy student who has frequent patient contact. She drinks alcohol occasionally but denies smoking and illicit drug use; she says she is not sexually active.
A 47-year-old Hispanic woman with severe headaches of 1 month’s duration presents to the emergency department (ED). The pain encompasses the entire head, is constant and crushing (10 on a scale of 1 to 10), and has progressively worsened.
Two weeks before admission, he had visited the emergency department (ED) because of the headache. Migraine was diagnosed and ibuprofen had been prescribed. The headache persisted despite NSAID therapy, and the patient returned to the ED 2 days later.
A previously healthy 16-year-old boy presents for evaluation of a slightly pruritic, nontender, generalized rash.

Six days ago, a 36-year-old man had noticed a dark spot in the field of vision of his left eye. Now the spot more closely resembled a line. He denied other changes in his vision and had not seen any floaters or flashing lights.
A 14-year-old boy presents with frequent severe headaches characterized by sharp, throbbing pain behind his left eye and left temple.
A 28-year-old woman presents with milky discharge in both breasts and throbbing occipital headaches of 4 months' duration. The headaches begin gradually, do not radiate, and have no apparent triggers or relieving factors.
I have read both that the male brain has no estrogen receptors and that testosterone is converted to estrogen in the brain. Where does the truth lie? And what role, if any, does estrogen play in preventing Alzheimer disease in both men and women?
Depression was diagnosed 6 years earlier in a 37-year-old woman; it has been successfully managed since then with fluoxetine and outpatient psychotherapy. Since her teenage years, the patient has also experienced sporadic (fewer than 3 or 4 per year) mild or occasionally severe headaches, which she has usually self-treated with over-thecounter (OTC) agents or "just slept off."
The development of more sophisticated testing modalities now permits the identification of coronary artery narrowing in asymptomatic adults. The images obtained in these studies provide potential targets for intervention-based therapy.
A 47-year-old woman complains of severe headaches that involve only the right orbital, temporal, and occipital areas. She describes the pain as sharp and stabbing, and she rates its severity as 9 or 10 on a 10-point visual analog scale.
LONDON -- Headache patients receiving prophylactic high-dose verapamil face a risk of heart rhythm disturbances that warrants EKG monitoring of all patients on the therapy, investigators here concluded.
A 50-year-old man with end-stage renal disease secondary to long-standing hypertension had an elevated hematocrit and progressively increasing hemoglobin levels. For the past 7 years, he had been receiving hemodialysis 3 times a week. He denied headache, flushing, easy bruising, bleeding, nausea, vomiting, chest pain, dyspnea, and other symptoms. He was not receiving exogenous erythropoietin.
The headaches vary in severity, but she usually has severeheadaches (8 on a 10-point visual analog scale[VAS]) once or twice a week; she describes the latter assevere throbbing or pounding pain on the top of thehead but also involving the occipital and frontalareas and occasionally one or the other temple.
A 24-year-old woman presents to the emergency department (ED) withgeneralized weakness, headache, and muscle cramping that have progressivelyworsened over the past week. Recently, she has also had nauseaand vomiting. She denies chest pain, palpitations, dyspnea, cough, fever,chills, diarrhea, and urinary symptoms. She has a history of type 1 renaltubular acidosis.
Advertisement
Advertisement
Trending on Patient Care Online
1
FDA Approves SimpleScreen CRC Blood Test for Colorectal Cancer Screening
2
Bepirovirsen and the Push to Close Hepatitis B Care Gaps
3
Noninvasive Testing and the Colorectal Cancer Screening Gap, With Mark Fendrick, MD
4
FDA Grants Fast Track Designation to HTX-001 for Symptomatic Nonobstructive Hypertrophic Cardiomyopathy
5