
























































































































































































How to assess the degree of cognitive impairment in your MS patient if you work outside of a major medical center and have little access to experts trained to administer cognitive tests? BICAMS can help. Details from an expert here.
Neurology
Latest News
Advertisement
Advertisement
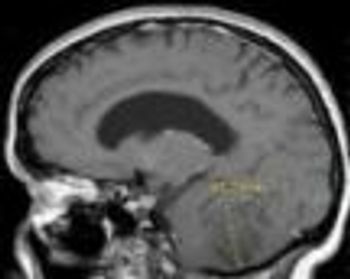
Lhermitte-Duclos disease is a rare, slow-growing, benign lesion of the cerebellum and is considered a hamartomatous tumor of the cerebellar cortex.
Common MS exacerbation triggers: infection, vaccination, stress, smoking, vitamin deficiency, or environmental changes.

Vertebral artery dissection may be misdiagnosed as post-concussive syndrome, stroke, or TIA, based on neurologic symptoms. Always consider after neck trauma.

Use of aspirin in primary prevention of cardiovascular disease must be based on individual risk-benefit analysis and is not appropriate for patients at low risk.

Medication overuse headache can result from overuse of any drug to abort acute headache. Discontinuation is the only effective treatment and is difficult.
The European Society of Cardiology just weighed in on the 3 new alternatives to warfarin for oral anticoagulation. The response is tempered enthusiasm.
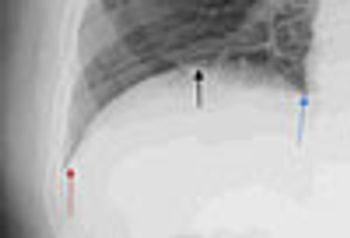
Phrenic nerve paralysis can present with chest wall pain, cough, and exertional dyspnea mimicking cardiac dyspnea. Fluoroscopy is the most reliable way to document diaphragmatic paralysis, and the sniff test confirms that abnormal hemidiaphragm excursion is due to paralysis rather than unilateral weakness.
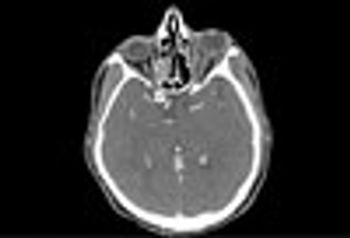
A 58-year-old man with a past medical history of chronic sinus disease and hypothyroidism presented with left periorbital pain and erythema that worsened despite outpatient treatment with topical antibiotics. An outpatient CT scan showed pansinusitis and orbital stranding. The diagnosis was orbital cellulitis and sinusitis.

A 4-year history of headache and severe neck pain led to a diagnosis of Chiari I malformation in this patient. Here: symptoms, diagnostic tests, and treatment approaches.

Here: 10 tips that can help you provide optimal care of your patients with MS.



In many patients, episodic migraines increase in frequency and transform into a refractory pattern.
What are the factors that underlie the transformation of episodic migraine to refractory migraine? Dr Susan Hutchinson explains.
A bad ("sick" or killer) headache is usually a migraine if underlying organic causes of pain are ruled out.
When counting sheep fails as first line therapy, what measures can you recommend to help your patient get some sleep?

In Part 2 of this podcast series, Dr Smith continues his discussion of the practice of nonsuicidal self-injury in adolescents.
Early differentiation of epileptic from nonepileptic seizures is important. Clues that suggest epilepsy are a history of febrile seizures (particularly if prolonged), past brain injury from trauma or infection, and epilepsy in first-degree relatives.
In this podcast, Dr Smith discusses the practice of nonsuicidal self-injury in adolescents-cutting, burning, self-hitting or banging, scratching, interfering with wound healing-may be increasing.
A 59-year-old woman had aphasia and right-sided weakness after a routine total knee replacement. CT and MRI scans revealed a large left middle cerebral artery infarct. A CT angiogram showed no significant disease of the cerebrovascular arteries. Test results for the lupus anticoagulant were positive. A venous study of the legs showed no deep venous thrombosis. She was treated with warfarin and aspirin and discharged. After speech and physical therapy, she had mild residual aphasia.
Psychiatrist Sidney Zisook, MD-a guest speaker at the recent American College of Physicians meeting in San Diego
Warm weather can impair the ability of persons with multiple sclerosis (MS) to learn, remember, and process information, according to research presented at the American Academy of Neurology’s 63rd Annual Meeting in Honolulu April 9 to April 16, 2011
Multiple sclerosis (MS) is less likely to develop in persons with high levels of sun exposure and vitamin D, reported Australian researchers in the journal Neurology. This finding confirms the results of previous studies that showed MS occurs more frequently at latitudes farther from the equator
Cannabis worsens cognitive function in patients with multiple sclerosis, reported investigators recently in the journal Neurology. Marijuana has been used to relieve the pain and spasticity associated with MS; however, the results of this study show that the drawbacks may outweigh the purported benefits
Advertisement
Advertisement
Trending on Patient Care Online
1
7 Drugs Approved for Primary Care: Q2 2026
2
FDA Clears OTC Adapalene-Benzoyl Peroxide Gel for Acne in Patients 12 and Older
3
Integrating Sleep and Life’s Essential 8 Into Cardiometabolic Care, With Michael Grandner, PhD
4
Tralokinumab Phase 2 TRAPEDS-1 Trial Shows Consistent PK, Safety in Children With Atopic Dermatitis
5