
London-based GlaxoSmithKline (GSK) plc and New York–based Pfizer Inc have announced they will combine their HIV drug divisions into a new company (Kelley T. Bloomberg News. April 16, 2009). GSK will hold an 85% share of the joint venture; Pfizer will hold 15%. According to a filing with the US Securities and Exchange Commission, GSK Senior Vice President Dominique Limet, a physician, is CEO-designate of the new company.
All News
Advertisement
Advertisement
The lifetime cumulative risk of at least 1 abnormal ocular lesion for an HIV-positive person ranges from 52% to 100%. Ophthalmic involvement can occur during the early phase of HIV infection, and ocular lesions are mainly noted in the posterior segment.1,2

A 58-year-old man with type 2 diabetes, nephrolithiasis, and benign prostatic hyperplasia presented with bilateral periorbital ecchymoses and left subconjunctival hemorrhage. The ecchymoses had spontaneously appeared 3 days earlier; the patient had no history of trauma or falls. He also had difficulty in voiding, characterized by increased frequency, hesitancy, and diminished urine stream.
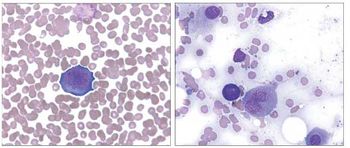
Persons with HIV infection frequently present with anemia from different causes, including use of antiretroviral therapy (typically zidovudine), iron deficiency, vitamin B12 deficiency, opportunistic infections (such as mycobacterial and fungal infections), chronic disease, AIDS-associated malignancies, autoimmune hemolysis, and direct effects of HIV infection itself. A frequently overlooked cause of chronic anemia in HIV-infected persons is parvovirus B19 coinfection.1-3 We present an illustrative case of unsuspected treatable parvovirus B19 infection in an HIV-positive person with chronic transfusion-dependent anemia initially attributed solely to zidovudine therapy.
Scrub typhus, which is caused by Orientia tsutsugamushi, has various systemic manifestations, including GI symptoms. We describe one patient with scrub typhus who presented with symptoms that suggested acute appendicitis and another who presented with symptoms of acute cholecystitis.
The human papilloma viruses (HPVs) are among the widespread sexually transmitted pathogens infecting women. Like HIV, HPV–s
Clostridium difficile infections account for most cases of antibiotic-associated colitis.1 However, there is increasing evidence that Klebsiella oxytoca infection contributes to the development of C difficile–negative antibiotic-associated hemorrhagic colitis. Most cases have been reported in France,2-12
A TOPICAL TREATMENT THAT KILLS herpes simplex virus type 2 (HSV-2) and that has long staying power may be available in the future. The experimental microbicidal solution, consisting of cholesterol-conjugated small interfering RNA (chol-siRNA), was tested in female mice that were given a lethal dose of the virus. The solution, delivered intravaginally, had a remarkably protective effect.
With the FDA approval of a new small-molecule drug to treat HIV infection by blocking the CCR5 chemokine receptor and with several other drugs of this class in development for this and other indications, there is an increased interest in determining the potential influence on tumor promotion or suppression that blocking this receptor may have. Large, long-term clinical studies would be the ideal method for evaluating the potential increase in cancer risk, and at least one such study is under way (see http://clinicaltrials.gov/show/NCT00665561?order=49).
Disseminated echinococcal disease can present complex management issues that require a multidisciplinary approach to care. We describe a patient with hydatid disease who had multiple cysts in the liver, lungs, and pulmonary artery that were caused by Echinococcus granulosus infection.
Advertisement
Should ART be deferred in patients at risk for nonadherence?Since nonadherence to antiretroviral therapy (ART) may hasten the development of resistance, it may seem reasonable to defer ART in HIV-infected patients who have risk factors for nonadherence, such as substance abuse.
A milestone has been reached in the treatment of sepsis—the institution of protocolized management that starts in the emergency department. Early goal-directed therapy, with targeted fluid resuscitation and measures of oxygen delivery, has been shown to improve survival in patients with septic shock. Although initiating aggressive fluid resuscitation is the first priority, it is also essential to rapidly obtain cultures and infuse broad-spectrum antibiotics. Norepinephrine is a more potent vasoconstrictor than dopamine and may be more effective in treating hypotension in patients with septic shock. Vasopressin is an effective second-line agent. Treatment with recombinant human activated protein C at 24 µg/kg/h for 96 hours has been shown to reduce mortality in patients with sepsis; its benefit is greatest in the most acutely ill patients. (J Respir Dis. 2009;30(1-2))
A 30-year-old white man with HIV infection since September 2004 presented to his infectious disease physician in January 2007 to restart his antiretroviral therapy. Three months earlier, he had discontinued all of his antiretroviral medications because of his loss of health insurance. He remained asymptomatic during this period, with the exception of some mild oral candidiasis. At the time of restarting his antiretroviral therapy, his CD4+ cell count was 264/µL and test results were positive for syphilis (rapid plasma reagent [RPR] titer of 1:128, confirmed with a fluorescent treponemal antibody absorption test).
Tenofovir disoproxil fumarate is extensively used for treatment of HIV infection. In addition, tenofovir has recently obtained FDA approval for treatment of hepatitis B, and it can therefore be assumed that this drug will be increasingly used in non–HIV-infected persons as well. Although the risk for nephrotoxicity with this agent is low, its widespread use will no doubt lead to more episodes of renal impairment in patients worldwide. It is important to identify those patients for whom tenofovir should not be used or, at the least, identify those patients, both HIV-infected and non–HIV-infected, for whom renal function should be more closely monitored during tenofovir use.
Tenofovir disoproxil fumarate is a nucleotide reverse transcriptase inhibitor that is usually well tolerated with few adverse effects, but it has been implicated in the development of Fanconi syndrome and renal insufficiency because of its effects on the proximal renal tubule. Vancomycin nephrotoxicity is infrequent but may result from coadministration with other nephrotoxic agents, such as aminoglycosides. We report the cases of 2 patients receiving tenofovir as part of an antiretroviral regimen in whom renal failure developed after a prolonged course of vancomycin.
Jake” was a 17-year-old high school student who came to see me with his supportive but anxious mother. Four months earlier, Jake’s pediatrician, having read the CDC recommendations for routine testing of all patients aged 13 to 64,
For 2009, 1,479,350 new cases of cancer, up from 1,437,180 new cases in 2008, are expected to be diagnosed in the United States, according to the American Cancer Society’s annual Cancer Facts and Figures report. About 562,340 deaths from cancer are forecast for 2009, a decrease from the 2008 estimate of 565,650 deaths. Cancer is the second leading cause of death in the United States (22.8%), exceeded only by heart disease (26.6%), and is responsible for nearly 1 of every 4 deaths among Americans.
As readers of April’s column titled “Surge in Mental Health Conditions in War Veterans” know, posttraumatic stress disorder (PTSD) is a problem for many military veterans returning from Iraq and Afghanistan. PTSD is also a significant issue in civilian life, where it affects more women than men, and is usually precipitated by physical attack, adult rape, or even childhood sexual molestation.1,2
About two-thirds (66.8%) of primary care physicians (PCPs) in the United States have difficulty obtaining outpatient mental health services for their patients-a rate more than twice as high as rates for other services-according to study findings published online April 9 in Health Affairs. The study was conducted by Peter J. Cunningham, PhD, senior fellow at the Center for Studying Health System Change (HSC), Washington, DC, and funded by the Commonwealth Fund.
A proposal for a pilot project to save money for a health plan was developed collaboratively with a clinic manager and the medical director of a local clinic. The goal was to encourage and support physicians in changing the proton pump inhibitor (PPI) medication prescribed for patients from a brand-name PPI to omeprazole, a more cost-effective generic option. The health plan identified members who had filled a prescription for a brand-name PPI and asked their physicians to consider switching the patients’ therapy to omeprazole. If the physician agreed to the change, the clinic would then send a letter to the patient, in which the physician recommended the change along with a new prescription for omeprazole. Following successful implementation in the initial pilot clinic, the program was extended to 4 more clinics. After achieving significant cost savings at all 5 clinics, the health plan is now expanding the program to more clinics as well as considering launching similar programs targeting other medication classes. (Drug Benefit Trends. 2009;21:158-163)
Advertisement
Advertisement
Advertisement