

























































































































































According to the Sgarbossa criteria, the patient had an acute MI: ECG revealed a greater than 1-mm ST-segment depression in lead V2 and about 5-mm discordant ST-segment elevation in leads II, III, and aVF.
Cardiology
Latest News

Advertisement
Advertisement
Clinicians sometimes give patients a choice of medication or lifestyle changes to control blood pressure (BP) or cholesterol levels.

Up to 40% of patients who present with what may look like simple, isolated superficial venous thrombosis have concomitant deep venous thrombosis. This finding has led clinicians to first rule out DVT bilaterally via compression Doppler ultrasonography before treatment is considered.
A 92-year-old woman presented with signs and symptoms of heart failure, including marked bilateral lower extremity edema, jugular vein distention, and difficulty in breathing at rest. Her medical history was significant for hyperthyroidism, chronic asthmatic bronchitis, and senile dementia. Medications included oral methimazole, 10 mg/d, and oral theophylline, 200 mg/d.
Case 1: Mr A. is a 55-year-old man who comes to your office for a routine physical examination. He is a traveling salesman and has recently gained weight. He does not exercise much and is a frequent visitor to fastfood establishments. His father had “a touch of diabetes” and died of a myocardial infarction (MI) at age 59.
Chest pain and dyspnea of acute onset prompted a 49-year-old man to seek urgent medical attention. Two months earlier, he had sustained fractures to the right arm and both ankles after a 25-ft fall. Ten days before presentation, the patient’s rehabilitation physician had discontinued daily enoxaparin because of improved mobility and a presumed decreased risk of thromboembolism.
A 59-year-old man presented with painful paraparesis of acute onset, severe low back pain, and shortness of breath. On initial examination, he had 0/5 strength and numbness in his lower extremities. The skin from below his umbilicus to his lower legs was pale.

Palpitations and dizziness prompted a previously healthy 21-year-old cable lineman from southeastern Pennsylvania to seek medical attention. An ECG showed first-degree heart block. The young man was scheduled for outpatient cardiology consultation, but his symptoms worsened and he presented to an emergency department with chest pain and fever 2 days later. Further evaluation revealed that for the past 3 weeks he had myalgia; arthralgia; fatigue; and an expanding, erythematous, nonpruritic rash on his trunk and extremities. He did not recall any tick bites.

Osler nodes may accompany bacteremia without endocarditis, septic endarteritis, typhoid fever, gonococcemia, systemic lupus erythematosus, and nonbacterial thrombotic endocarditis.
Ventricular versus supraventricular tachycardia? This case offers diagnostic and treatment strategies when the diagnosis is uncertain.
Kawasaki syndrome is a serious disorder affecting children aged 1 to 8 years. It mimics a range of other diseasesof childhood. Diagnosis is based on physical examination findings coupled with the exclusion of other causes.
A 27-year-old woman with hypertension, type 1 diabetes mellitus, and end-stage renal disease presents to an outpatient renal clinic complaining of generalized weakness. She missed her last dialysis session 2 days earlier.

The morning after an 88-year-old woman with symptomatic second-degree type I (Wenckebach) atrioventricular block underwent placement of a dual chamber pacemaker without complication, she awoke with uncomfortable pulsations in her abdomen. The pacing thresholds and impedance had remained unchanged since implantation.
Systolic hypertension is an independent risk factor for coronary artery disease, stroke, and end-stage renal disease. Nonpharmacological interventions for systolic hypertension include limitation of dietary sodium and alcohol intake along with weight reduction and aerobic exercise.
A 57-year-old woman presents for follow-up several months after a series of thrombotic episodes. Four days after she underwent ankle fusion to relieve pain and edema associated with a leg fracture that had occurred 40 years earlier, she sustained a massive myocardial infarction (MI).
In medicine, for far too long, men and women were lumped together into "one size fits all" algorithms or, worse, women were presumed to be smaller versions of their male counterparts.

An obese 61-year-old man with a history of heroin abuse was brought to the hospital after he had fallen onto his buttocks on a sidewalk. He was able to stand initially, but weakness and numb-ness in his legs rendered him suddenly unable to walk or prevent himself from voiding. He denied abdominal or back pain. His medical history included asthma, chronic obstructive pulmonary disease, and hypertension.
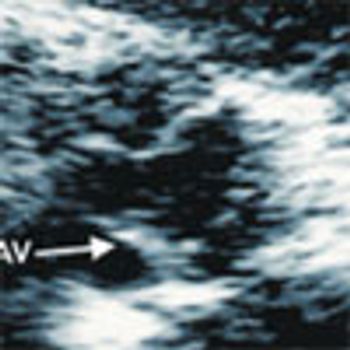
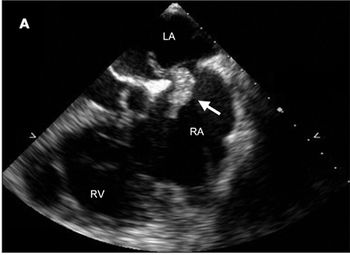
In recognition of Valentine's Day, we present 2 incidental heart-shaped findings we encountered within the hearts of 2 patients during 2-dimensional transthoracic echocardiographic studies.
With patients who say that they usually faint when blood is drawn or when given an injection, have them lie down and tell them that they "cannot faint when lying down." Whether for physiological or psychological reasons, patients usually do not faint when this is done.
To help answer the question of Mary Ellen Lewis, PA-C, about her patient with a low-density lipoprotein (LDL) cholesterol level of 120 mg/dL and a high-density lipoprotein (HDL) cholesterol level of 100 mg/dL(CONSULTANT, June 2007), I would like to describe my approach to the treatment of dyslipidemia.
A 62-year-old man presents with painful cramps in his left lower leg that began about 6 months earlier and have recently become more frequent. The cramps occur with vigorous walking and cease when he stops for several minutes.
Nephropathy develops in about 30% of patients with diabetes. Screen for albuminuria at the time type 2 diabetes is diagnosed and within 5 years of diagnosis of type 1 diabetes.
During the first quarter of a football game, a 17-year-old athlete noticed that his right (dominant) arm was swollen and heavy. Two days earlier, he had fired a shotgun right-handed multiple times while hunting.
An oral renin inhibitor, aliskiren, recently became available. Does it have any advantages over angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs)?
When angiotensin-converting enzyme (ACE) inhibitors were first discovered, they were a welcome addition to the antihypertensive armamentarium. Since then, many more benefits of these drugs have been found: they slow the progression of diabetic nephropathy, abate the sequelae of heart failure when systolic dysfunction is present, and reduce the level of proteinuria in patients with nephrotic syndrome.
Advertisement
Advertisement
Trending on Patient Care Online
1
ACOG Releases New Guidance on HIV Screening and Prevention
2
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
3
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
4
FDA Approves First Oral PCSK9 Inhibitor to Reduce LDL-C in Adults With Hypercholesterolemia
5