
• Search images and case studies of conditions submitted by physicians • Browse by anatomy, image type, or diagnosis • Use high-resolution images to improve diagnostics • Click on any diagnosis to learn about symptoms and treatment • Bookmark images
All News
Advertisement
Advertisement
Obesity is associated with a broad range of GI health risks. An expert panel discussed these risks, which were documented in abstracts presented at the 2010 ACG Scientific Meeting.
Hands-on sessions markedly enhance the CME experience. New to the ACG Scientific Meeting in 2010, the hands-on workshop center proved to be one of the conference’s most popular offerings.
The ACG 75th Annual Scientific Meeting provides an overview of recent advances in the diagnosis and treatment of various GI disorders, ranging from ulcerative colitis to fructose intolerance in children. ConsultantLive has captured the highlights of the meeting with reports on key presentations.
Advertisement
Since continuing technological advancements are going to add to rising costs (dialysis, for example, with more “baby boomers” coming of Medicare age), one has to wonder what the something is that “has to give” in the future.
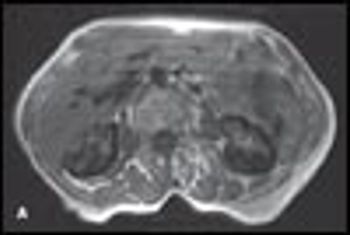
MRI scans of the kidneys of an 83-year-old woman with history of myelodysplastic syndrome are shown. Normal MRI scans are shown for comparison. The patient had intermittent episodes of dark-colored urine for years. Findings from repeated cystoscopies were normal.
A 48-year-old woman sought medical attention after an episode of gross hematuria associated with mild right-sided loin discomfort. She did not have urinary frequency, urgency, or dysuria. Her history included 3 urinary tract infections; a Proteus species was cultured on each occasion. The family history was unremarkable. Other than mild loin tenderness, physical findings were normal.
Patients' descriptions of their medications can cause confusion-with potentially dangerous results.
Advertisement
Advertisement
Advertisement