































































































































































A 63-year-old woman presents withdiffuse hyperkeratosis of the solesand palms. She also has onycholysis-separation of the nail plate fromthe nail bed-and salmon-coloredplaques behind her ears. Biopsy ofone of the plaques confirms the suspecteddiagnosis of psoriasis.
Infectious Disease
Latest News
Advertisement
Advertisement
A middle-aged man with"jock itch" that has failed torespond to antifungal creams.An older woman who has diffusehyperkeratosis of predominantlyweight-bearing surfaces.A young man with mildlypruritic, small, salmon pinkpapules and thick white scaleon his trunk and arms.
A 30-year-old man presents with scalingand erythema of the scalp that extendspast the anterior hairline. Thepatient has a family history of psoriasis.For the past 5 years, he has experiencedwintertime flares of the diseasethat affect his scalp and the extensorsurfaces of the extremities.
A 46-year-old man complains that his"jock itch" failed to respond to antifungalcreams. The patient has hadpsoriasis on his elbows and knees formany years.
A 72-year-old man presents with skinlesions and nail abnormalities. Erythematous,sharply defined, demarcatedpapules and rounded plaquescovered by silvery micaceous scaleare noted on the elbows, knees, andscalp. Involved areas appear to be bilaterallysymmetric. Localized psoriasisvulgaris is diagnosed.
4A:Small, slightly pruritic, salmonpink papules with thick white scalehave arisen over the past 5 days onthe trunk and arms of a 24-year-oldman. The patient has a history ofvery mild psoriasis vulgaris of the elbows,knees, and scalp; he deniesstreptococcal pharyngitis or other recentinfections. Guttate psoriasis isdiagnosed.
Focal, painless discoloration of theleft thumbnail (A) developed severalyears earlier in this 46-year-old man.Oral antifungal therapy had no effecton the lesion.
A 35-year-old man presents with extensiveplaques over much of thetrunk and extremities. This severeflare of psoriasis developed after astressful emotional experience.
A 60-year-old man with a long historyof psoriasis vulgaris required a systemiccorticosteroid for a severe exacerbationof asthma. Soon after theErythrodermic or Pustular Psoriasiscorticosteroid was discontinued, generalizederythema and scaling of theskin developed.

A 38-year-old man presented with a fleshy lesion beneath the tip of his penis. He had discovered it about 18 months before the initial evaluation. A second similar lesion resembling a “cauliflower” had appeared several weeks after the first. Both lesions had grown and had begun to bleed during intercourse.

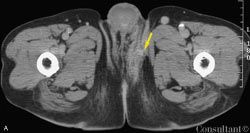
A 40-year-old man presented with a 5-year history of progressively increasing bilateral leg swelling that was neither painful nor pruritic. There was no history of dyspnea, jaundice, or groin surgery. The patient reported multiple previous episodes of superimposed cellulitis, which were treated with antibiotics. There was no family history of similar illness.
ABSTRACT: In addition to advanced age, factors such as comorbid illness and debility determine the risk of community- acquired pneumonia (CAP). Many elderly persons do not have the classic symptoms of CAP; instead, they may present with confusion, lethargy, tachypnea, anorexia, or abdominal pain. Even with thorough investigation, an infectious pathogen can be identified in only about half of patients. In addition to the causative organisms for pneumonia in younger adults, elderly persons are at risk for infection with organisms such as Haemophilus influenzae, Staphylococcus aureus, enteric gram-negative bacteria, and anaerobes, and for polymicrobial infection. Prompt empiric treatment is essential. Recommended initial therapy choices include a ß-lactam agent with a macrolide, or an antipneumococcal fluoroquinolone.

Bullae had recently appeared on the dorsa of the hands and fingers of a 46-year-old man. His medical history was significant for alcoholism, discoid lupus erythematosus (DLE), and hepatitis C. Systemic lupus erythematosus (SLE) was ruled out; the patient’s symptoms did not meet the American Rheumatism Association criteria for SLE.
For several days, a 60-year-old woman has had fever, myalgias,fatigue, poor appetite, and diminished oral intake. Shedenies cough, sputum production, and urinary symptoms.
A blue-black nodule has been present next to a 19-year-old woman’s left eyesince birth. After recent accidental trauma, the lesion has enlarged.
ABSTRACT: Recent evidence suggests that viral infection is the most likely underlying cause of Bell's palsy. Rapidity of onset is a clue to the diagnosis; unilateral facial weakness or paralysis develops over 24 to 48 hours. Rule out other causes of peripheral facial paralysis, such as Ramsay Hunt syndrome and Lyme disease. Although most cases of Bell's palsy resolve without medical or surgical intervention, older patients and those with abnormal electroneurographic results are less likely to have complete recovery of facial function. Early treatment with an oral corticosteroid is likely to enhance recovery; concurrent use of acyclovir may also be helpful. Surgical decompression has been effective in patients with abnormal electroneurographic results.

Several lesions had appeared 1 week earlier on the left distal thigh of a 47-year-old woman. The affected area featured erythema with irregular faded borders and central redness with very fine papules over the L3 dermatome. The indurated and tender central areas suggested inflammation or necrosis. There were no vesicles and there was no drainage.
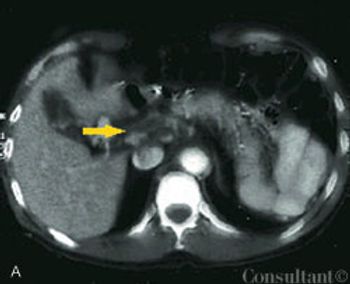
A 60-year-old man presented to the emergency department (ED) with fever of 1 day’s duration and midabdominal pain. The cramping pain had begun 3 days earlier in a bandlike distribution around the upper abdomen. Ingestion of food exacerbated the discomfort. The patient had a history of intermittent constipation; he denied alcohol or illicit drug use, nausea, vomiting, and weight loss. He did not use any herbal or over-the-counter medications.
ABSTRACT: Serum levels of aspartate aminotransferase and alanine aminotransferase that exceed 1000 IU/L indicate acute viral hepatitis (A, B and, rarely, C), acute drug toxicity (eg, acetaminophen overdose or isoniazid hepatotoxicity), or ischemic liver injury. In chronic hepatitis (ie, hepatitis B or C or autoimmune), values range from mildly elevated to usually less than 400 IU/L. Elevated levels of alkaline phosphatase and gamma;-glutamyltransferase (GGT) are consistent with cholestatic disease: primary biliary cirrhosis, primary sclerosing cholangitis, idiosyncratic drug reactions, or mechanical biliary obstruction (eg, biliary stones or tumor). Elevation in the GGT level can also be induced by alcohol consumption or medications (eg, phenytoin). Isolated unconjugated hyperbilirubinemia suggests Gilbert syndrome or a hematologic disorder; conjugated hyperbilirubinemia reflects impaired hepatic excretion. Serum bilirubin and albumin and INR have prognostic significance in chronic liver disease; bilirubin and INR are more useful in acute liver failure because albumin has a long half-life.
A 12-month-old infant is brought to your office for evaluation of ared, swollen left index finger, which her parents first noted the prior evening.The mother denies any known trauma or recent illness. She tells you that theinfant is slightly fussy and is not taking her bottle as well as usual.
A network of purplish pink lesions recently developed on a 28-year-old woman’sarms and legs. The asymptomatic rash becomes more prominent with exposureto cold. The patient denies fever, aches, arthralgias, oral erosions, chestpain, and photosensitivity.
Sir William Osler once called pneumococcalpneumonia “the captain of themen of death.”1 Pneumonia is the sixthleading cause of death in the UnitedStates and the fourth leading causeamong Americans 80 years of age andolder.2
A 47-year-old woman who wasseropositive for HIV-1 presented tothe emergency department with severemaculopapular, erythematouseruptions. Her antiviral regimen hadrecently been changed from zidovudine, 300 mg bid; lamivudine, 150 mgbid; and saquinavir, 600 mg tid, tolamivudine, 150 mg bid; stavudine, 40mg bid; and nevirapine, 200 mg/d.
A 64-year-old man underwent a right pneumonectomy forsquamous cell carcinoma of the right lung. He was dischargedfrom the hospital on the fifth day after surgery.
Three weeks after coronary artery bypass graft (CABG)surgery, a 52-year-old woman complained of pain at thesternal scar. The patient had a history of diabetes and hypertension.She had smoked cigarettes for many years.
Advertisement
Advertisement
Trending on Patient Care Online
1
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
2
FDA Approves First Oral PCSK9 Inhibitor to Reduce LDL-C in Adults With Hypercholesterolemia
3
FDA Accepts Cefiderocol sNDA for Pediatric Gram-Negative Infections
4
Subcutaneous Lecanemab Shows Comparable Exposure in Early Alzheimer Disease
5