Charles E. Crutchfield III, MD
Articles by Charles E. Crutchfield III, MD
Although tinea versicolor is fairly common, its appearance on the face and neck is unusual, notes Robert P. Blereau, MD of Morgan City, La. His patient, a 30-year-old woman, exhibits the pale, rounded, fine-scaled lesions typically found on tanned or dark-skinned persons.

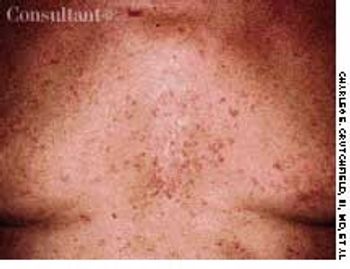
The sharp transitions in pigmentation on the anterior surface of the arms of this 49-year-old black man were noted as an incidental finding. The arms' lateral aspects were distinctly more deeply pigmented than the medial aspects. In addition, a hyperpigmented band was present over each pectoral area, while a hypopigmented vertical stripe covered the sternum. These symmetric transitions in pigmentation are normal variants found most commonly in blacks and are known as pigmentary demarcation lines.

This 19-month-old child exhibits the characteristic features of hypomelanosis of Ito, a neurocutaneous disorder.

A 48-year-old man requested medical evaluation of the multiple spots that gradually appeared on his legs over the past 5 years.

Flat, tan-pink patches on his lower legs disturbed a 52-year-old man. The lesions had visible, nonpalpable petechiae, which did not blanch on diascopy; telangiectasia and inflammatory vasodilation, therefore, were excluded from consideration.

Flesh-colored to red-brown nonpruritic papules developed most prominently on the elbows, forearms, and knees of a 2 1⁄2-year-old boy. The rash was preceded by a low-grade fever and mild, upper respiratory tract symptoms.
our years ago, this patient had necrotizing cellulitis of the right calf that required surgical debridement. He did well for the next 2 years, but then his lower leg became increasingly swollen.

A 69-year-old woman, who was being seen regularly for treatment of psoriasis, was noted to have numerous open comedones on the sides of her face in association with photodamaged skin.

After having been bothered by these lesions for the past 9 months, a 27-year-old woman described the eruption as "itchy bumps under my arms."

A 23-year-old man complained of unsightly “flat warts” all over his chest. These lesions first appeared in early adolescence. The clinical suspicion of epidermodysplasia verruciformis was confirmed by a biopsy.

A 61-year-old man with a history of squamous cell carcinoma was concerned about a tender nodule on his ear. He complained of exquisite tenderness with pressure, such as when lying on the affected side at night.

A 24-year-old man presented for evaluation of pruritic vesicles on both feet. Ten days earlier, dyshidrotic eczema had been diagnosed by another physician who prescribed triamcinolone ointment. The patient reported that the foot eruption worsened after the topical medication was applied.

A recent outbreak of small-plaque and guttate psoriasis was confined primarily to the arms of this 32-year-old woman. The slightly scaly, brick-red, linear plaques and clusters consisted of 3- to 10-mm papules, some of which were surrounded by a faint whitish ring. It was quickly ascertained that many of these lesions corresponded to areas where the patient had been scratched by her cat.

Referral for biopsy was made because a 6-mm, red and black, dome-shaped papule on a 43-year-old woman's left groin resembled a melanoma. The patient had numerous cherry hemangiomas on her trunk-bright red, 2- to 5-mm papules that are among the most common vascular anomalies.

Concerned about this unsightly and painful lesion, a 34-year-old man asked to have it removed. The patient first noted this eruption on his back several months before. This lesion is an infundibular cyst.

A 57-year-old man with a history of venous stasis leg ulceration wondered about the “white spots” on his leg.

After more than 15 years of wondering what the “white specks” on his legs were, a 64-year-old man consulted his physician. The patient was taking medication to control hypertension; he was otherwise healthy.

Mongolian spots are benign, congenital blue-gray macules or patches commonly found in Asian, black, and Hispanic infants (and in 5% of white infants). They are most often located in the sacrogluteal area and the upper back. The lesions may be solitary or multiple, vary in color intensity, and frequently enlarge until about age 2, when they gradually fade and disappear. Approximately 5% persist into adulthood.

The dark red plaques seen here developed rapidly under both arms of this markedly obese 43-year-old woman. The lesions spread concentrically, forming necrotic ulcerations with overhanging borders, and there was surrounding violaceous discoloration. No other areas of the patient's body were involved, and she was otherwise in good health.

A 66-year-old man presented with numerous cutaneous tumors. He had dementia and thus was unable to provide an accurate history.

Five days after beginning aggressive treatment with intravenous corticosteroids for inflammatory bowel disease, this 26-year-old man noticed the sudden eruption of this mildly pruritic rash.

This contorted hand of a 49-year-old man demonstrates Dupuytren's contracture, a disorder first described by Baron Guillaume Dupuytren in 1831. Although the condition may occur as a completely independent abnormality, it is commonly associated with chronic liver disease, diabetes mellitus, epilepsy, palmar fasciitis, carpal tunnel syndrome, rheumatoid arthritis, pulmonary tuberculosis, and alcoholism. This patient had a history of alcohol abuse.

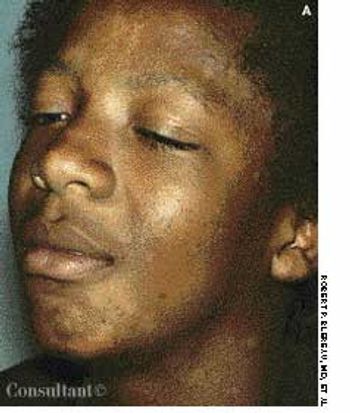
Loss of pigmentation is noted around the left eye of a 49-year-old African-American man-the same eye in which he has a detached retina. In addition, the patient's hearing is impaired on that side.

Severely limited vision plagues this 27-year-old woman with aniridia, the bilateral absence of the iris of the eye.
The lesions seen here developed shortly after a 54-year-old woman started psoralen plus UVA (PUVA) therapy for psoriasis. This is acne estivalis, an uncommon actinic, acneiform eruption. The firm, red, monomorphic papules are most commonly found on the shoulders, arms, neck, and chest. Histologically, they resemble steroid acne. Lesions develop in the spring, peak in the summer, and resolve in the fall without scarring.

Seen here are a 38-year-old Native American woman and her 20-year-old daughter, each of whom has had a relapsing eruption for several years. Pruritic, red to red-brown plaques develop on their faces and necks and on the dorsal surface of their hands. Scattered brown and hypopigmented macules as well as some scaling and slight erythema appear on their lower lips. The women stated that the eruptions flare each spring and gradually improve throughout the rest of the year. The daughter's lesions were more acute at this time and had developed during the preceding 3 days.
A 57-year-old man with a history of venous stasis leg ulcerationwondered about the “white spots” on his leg. Thecondition is atrophie blanche, which manifests as smooth,ivory-white macules and plaques of sclerosis stippled withtelangiectasia that often are surrounded by mild to moderatepigmentation.
A 24-year-old man presented for evaluation of pruritic vesicles on both feet.Ten days earlier, dyshidrotic eczema had been diagnosed by another physicianwho prescribed triamcinolone ointment. The patient reported that the footeruption worsened after the topical medication was applied.

For 3 years, a linear plaque had been slowly developing on the left palm of a 47-year-old woman who had difficulty in opening and closing her hand. There was no contributory family history.
Cutaneous manifestations develop inapproximately 30% of persons withdiabetes. Premature atherosclerosisis a common complication of thedisease and can cause peripheral infarction,ulceration, and necrosis.
