

This mobile tender nodule was discovered on the left wrist of a 60-year-old woman with a history of many non-melanoma skin cancers. What’s your best diagnostic guess?
This mobile tender nodule was discovered on the left wrist of a 60-year-old woman with a history of many non-melanoma skin cancers. What’s your best diagnostic guess?

These wounds occurred when this 77-year-old woman fell when chasing her dog. Such wounds-a combination of ecchymoses and erosion caused by blunt and sheering forces on fragile skin-are common in the elderly, even after relatively mild trauma. Simple interventions will promote healing.

These classic linear, wide-mouthed, red to purple, atrophic patches are classic for stretch marks (striae distensae). The patient was in the middle of his growth spurt.

The patient assumed that the itchy rash was due to insect bites. The shape, size, color, and presence of 6 legs of the insect he captured were consistent with bedbugs and bedbug bites.

The red patch on this woman's neck is lichenoid keratosis, a variant of seborrheic keratosis. Diagnostic contenders included Bowen disease and superficial basal cell carcinoma.

Both morphology and location favor the diagnosis of psoriasis. The presence of nail pitting, and a strongly positive family history for psoriasis, confirmed the diagnosis.

These widely scattered, dome-shaped pruritic inflammatory papules suggest insect bites. A biopsy showed mixed dermal infiltrate consisting of lymphocytes and eosinophils, consistent with an arthropod assault.

The differential diagnostic possibilities for this tender nodule included hypertrophic actinic keratosis, keratoacanthoma, squamous cell carcinoma, and verruca. The possibility of squamous cell carcinoma dictated removal with histologic examination.

A multiplicity of colors in a pigmented lesion usually dictates the need for a biopsy. In this woman with many nevi and a history of malignant melanoma, biopsy revealed an inflamed blue nevus and was also curative.

The development of eccentric pigmentation within a previously stable pigmented lesion may indicate malignant degeneration, as was the case here. Of all melanomas, lentigo maligna melanoma has the best overall prognosis.

Round plaques like this one, each composed of many small erythematous papules, are classic for granuloma annulare. Large numbers of these lesions and widespread distribution is often associated with diabetes mellitus.

Sebaceous hyperplasia are commonly mistaken for basal cell carcinoma. These small papules with a yellowish hue and central dell is typical of the former, for which no treatment is required.

Biopsy of this red, scaly patch showed in situ squamous cell carcinoma. Treatment consisted of once-daily topical application of 5% imiquimod until erosion occurred. This off-label treatment affords an excellent cosmetic result.

These small areas of white dyschromia are typical of white superficial onychomycosis, often due to dermatophyte invasion following minor trauma. This form of onychomycosis usually responds well to topical therapy.

This is a prototypical case of acute contact dermatitis to benzoyl peroxide that the patient had been applying for her mild to moderate papulo-pustular acne. Twice-daily application of hydrocortisone 2.5% cream led to prompt resolution of the rash.

Biopsy of the flat area of this erythematous patch revealed superficial basal cell carcinoma while biopsy of the more nodular component revealed deeply infiltrating basal cell carcinoma.

This non-tender, freely mobile, rubbery-feeling nodule is a classic lipoma. Diagnostic contenders include epidermal cyst and cutaneous metastases.

Eccentric and irregular pigmentation prompted a biopsy in this elderly woman with a history of basal cell carcinoma and melanoma. The surprising diagnosis was a heavily pigmented squamous cell carcinoma in situ.

Biopsies of this large variegated pigmented plaque ruled out lentigo maligna melanoma and gigantic seborrheic keratosis.

This translucent dark pink nodule located just behind the nail is the classic presentation of a digital myxoid cyst.

After a dog bite, trauma in the form of a subungual hematoma and shallow lacerations prompted a 10-day course of amoxicillin-clavulanate. This antibiotic is also useful for cat and human bites that appear to be at high risk of becoming infected.

A biopsy revealed non-caseating granulomata, and culture revealed Mycobacterium marinum. This patient had a fish tank at home, and used his right hand to perform maintenance.
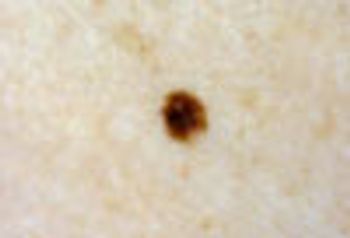
This pigmented macule clearly stands out against a bland background of fair-complected skin. This is known as the “ugly duckling” sign. Such lesions should always be viewed with suspicion and a biopsy is generally indicated.

This tumor is a low-grade soft tissue sarcoma. Metastases are uncommon, but local recurrence is very frequent. Mohs surgery is the optimal treatment modality.

The shallow ulceration surrounded by a ring of erythema is characteristic for aphthous ulcers (canker sores). This patient’s otherwise negative history rules out Behcet’s disease.

The persistent pigmentation on this woman’s hands corresponds to areas of intralesional injections of bleomycin for recalcitrant warts.
Because of this patient’s recent travel history to Africa, the penile lesions were cultured, and Haemophilus ducreyi was isolated, confirming the clinical suspicion of chancroid.

Adult-onset psoriasis is uncommon without a precipitating factor. In this patient’s case, an oral beta-blocker precipitated the psoriasis.

Contact dermatitis to paste-on fingernail decorations developed when the patient held her lower eyelid down with her index finger to insert her contact lenses.

This non-specific pruritic eruption is a common manifestation associated with HIV infection, especially in the pediatric population.

July 1st 2010
September 8th 2010

June 28th 2011

September 14th 2005
October 2nd 1999
October 2nd 1999