



























































































































































For a few months, a 51-year-old woman has had an asymptomatic rash on her proximal thighs. She claims to have no other rashes and denies any exposure history.
For a few months, a 51-year-old woman has had an asymptomatic rash on her proximal thighs. She claims to have no other rashes and denies any exposure history.

The mother of a 10-year-old boy brings him for evaluation of a persistent rash on his shins of a few months’ duration. The rash has not responded to topical corticosteroids.

For the past year, a 15-year-old boy has had a pruritic eruption on his shins. His mother suspects that his soccer shin guards are the cause; however, he wears them over his socks. Topical corticosteroids have not been effective.
More than 1 million persons in the United States may have been infected with novel H1N1 (swine) influenza virus, according to US health officials. In a recent media briefing, Dr Anne Schuchat, Director of the National Center for Immunization and Respiratory Diseases, CDC, noted that the infection is continuing to spread well past the typical influenza season in the Northern Hemisphere.
The World Health Organization (WHO) today declared the influenza A (H1N1) outbreak to be a pandemic. The agency decided to raise the pandemic alert level from Phase 5 to 6 based on the rising number of cases seen in Australia and Asia.
If Shakespeare were alive, he would urge caution regarding the “Ides of Influenza.” Recent publicity about global influenza, a result of both potential and real avian and swine flu epidemics, has led to a plethora of theories as well as alarm. How can the primary care practitioner answer questions, educate, prepare, and alleviate anxiety?
Sometimes we try to distill long experience into words, whether aphorisms or full paragraphs. Rilke’s wonderful prose poem expresses this very well in the part that begins, “For the sake of a single verse, one must see many cities, men and things. . . . ” While medicine has only some features in common with poetry, what reverberates is the wish to impart an affecting draught of beauty or wisdom or insight, in the case of poetry, after many years and decades of immersion in life; and I here offer some fruits of long observation and participation “hip deep” in clinical care and in the teaching of residents.

Osler nodes may accompany bacteremia without endocarditis, septic endarteritis, typhoid fever, gonococcemia, systemic lupus erythematosus, and nonbacterial thrombotic endocarditis.
Herpes simplex virus (HSV) infections are caused by 2 types of HSV: type 1 (HSV-1) and type 2 (HSV-2). Most cases of HSV infection are caused by HSV-2. Most persons with HSV-1 or HSV-2 infection have no or only minimal signs or symptoms. When signs do occur, they usually appear as one or more small blisters or sores on or around the mouth, lips, nose, face, genitals, and buttocks. HSV infections are very contagious and are spread by direct contact with the skin lesions.

For the past 5 years, a 30-year-old woman has had boils on her groin. She has tried at least 3 different antibiotics over the years, but none of them have been effective. She is otherwise healthy; the only medication she takes regularly is an oral contraceptive.
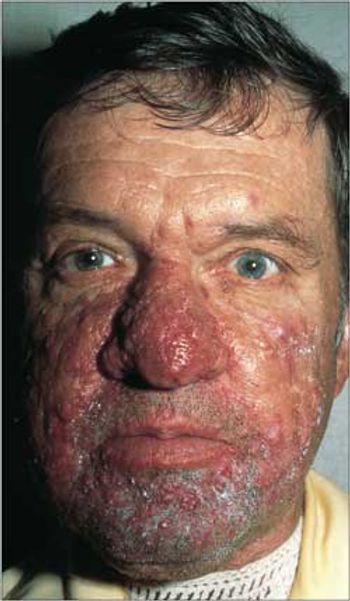
A 41-year-old man is seen for routine physical examination. Apart from mildly elevated cholesterol 2 years ago and a bout of bacterial bronchitis last winter, he has been healthy. Says he has had “bad acne” since age 21. Has applied drying agents that worsened it and that sting; has “sensitive skin” problems from creams. Now prefers to ignore his facial skin.

A 49-year-old man has had intermittent eruptions of itchy blisters on both of his palms for the past 15 years. The lesions heal after 2 to 3 weeks and then occur again after 6 months. He suspects that they are caused by poison ivy, but he is unsure of where he would have been exposed to the plant.
A milestone has been reached in the treatment of sepsis-the institution of protocolized management that starts in the emergency department. Early goal-directed therapy, with targeted fluid resuscitation and measures of oxygen delivery, has been shown to improve survival in patients with septic shock. Although initiating aggressive fluid resuscitation is the first priority, it is also essential to obtain cultures rapidly and infuse broad-spectrum antibiotics. Norepinephrine is a more potent vasoconstrictor than dopamine and may be more effective in treating hypotension in patients with septic shock. Vasopressin is an effective second-line agent. Treatment with recombinant human activated protein C at 24 µg/kg/h for 96 hours has been shown to reduce mortality in patients with sepsis; its benefit is greatest in the most acutely ill patients. (Infect Med. 2009;26):134-143)
If Shakespeare were alive, he would urge caution regarding the “Ides of Influenza.” Recent publicity about global influenza, a result of both potential and real avian and swine flu epidemics, has led to a plethora of theories as well as alarm.
During a flight from Houston to New York, a 46-year-old man had fever, chills, rigors, and body aches. After he landed, he sought treatment at a local hospital. The patient was on his way back to Liberia, where he works. He had been at home in Houston for several weeks. In the emergency department, he complained only of subjective fever.
For 1 week, a 77-year-old man had a fever and a tender, nonpruritic rash on both palms (Figure 1) and on the anterior aspect of both knees (Figure 2). Two weeks earlier, he had hives, which ameliorated after a 10-day course of cetirizine and a tapering course of prednisone. He also had headaches almost daily for the previous 6 to 8 weeks.
Here we provide a list of questions with links that can help you respond to patients who may be asking you about H1N1 virus infection (swine flu). Topics include travel restrictions and recommendations for persons with chronic disorders.

An 88-year-old man who had left hip repair after a fracture a few months earlier is now admitted to behavioral hospital because of implacable refusal to take medications, and because of poor food intake and ongoing refusal of rehabilitation. Ambulated with a walker before fracture but now barely ventures out of wheelchair even with rolling walker and therapist guidance.
In the United States, an estimated 5 million people have heart failure and about 550,000 new cases occur each year.1 The incidence is rising as more patients survive what were once fatal myocardial infarctions (MIs). Coronary artery disease (CAD) and hypertension are the most common causes of heart failure. The less frequent causes include diabetes; viral infections; valvular heart disease; drugs (eg, doxorubicin); and postpartum, alcoholic, and familial cardiomyopathies.2,3
About 50% of pregnanciesin the United States areunplanned.

For 1 month, a 54-year-old woman has had an intensely pruritic eruption on her abdomen, arms, and anterior thighs. She has long-standing hypertension and type 2 diabetes mellitus, which are treated with an angiotensin-converting enzyme inhibitor/diuretic and an oral hypoglycemic agent.

This worsening rash developed after a 40-year-old man was treated with amoxicillin for an upper respiratory tract infection. When the rash started, the amoxicillin was discontinued and azithromycin was prescribed; however, the rash has persisted. The patient has no history of allergies or rashes. He takes no other medications.
Multiple sclerosis patients treated with natalizumab risk reactivation of latent herpes virus infections.
Researchers have identified 2 gene variations that are resistant to interferon ß therapy. This finding could lead to a biomarker for determining when IFN-ß is appropriate for the treatment of multiple sclerosis.
Syphilis took Europe by storm at the end of the 15th century in what was to become a sweeping epidemic. Before 1495, it was unknown or perhaps was attributed to other disease processes, such as leprosy.