
























































































































































A 66-year-old woman was hospitalized because of severe anemia secondary to myelodysplastic syndrome. She had had associated fatigue and throbbing pain in both legs for several days.
Endocrinology
Latest News
Advertisement
Advertisement
Worsening painful ulcers on both legs prompted a 62-year-old woman to seek medical attention. She had a history of rheumatoid arthritis (RA), demonstrated by the markedly deformed interphalangeal joints in her thumbs (A), and scleroderma-polymyositis overlap syndrome.
A 74-year-old woman presented with a refractory pruritic eruption. Four months earlier, she had sought evaluation of a thickened, slightly crusted 6 3 8-cm patch on her right ankle of 2 months' duration. Contact dermatitis with secondary impetigo from scratching was suspected, and a topical corticosteroid and an oral antibiotic were prescribed.
Over the past 20 years, the treatment armamentarium for diabetes has greatly expanded: 8 different classes of non-insulin drugs and 8 different types of insulin are now available. The newer classes of agents include disaccharidase inhibitors, thiazolidinediones, meglitinides, glucagonlike peptide analogs, and dipeptidyl peptidase IV inhibitors.
BOURNEMOUTH, England-A campaign to urge kids to stop drinking sugared carbonated beverages-an effort to have them lose weight or prevent obesity-didn’t seem to have much value in the long run, reported investigators here.
WACOL, Australia-Schizophrenia leads to an age-related mortality rate that is about 2.5 times that of the general population, and the difference appears to be increasing, researchers here reported.
Here: a look at the many possible causes of poorly controlled blood glucose levels, and steps to overcome them.
ROCHESTER, NY-Breast cancer patients with a history of traumatic or stressful life events have a significantly increased risk of recurrent disease, investigators here have found.
DENVER-A higher intake of omega-3 fatty acids found in fish was linked to a lower risk of pancreatic islet autoimmunity in children at genetic risk for type 1 diabetes, according to a preliminary study.
SAN FRANCISCO-Oncologists may be able to predict which breast cancer patients need and will respond to systemic therapies with a single genomic profiling assay, researchers said.
SAN FRANCISCO-Biology, rather than access, income, or education, is the major driver of the well-known racial differences in breast cancer outcome, researchers reported here.
ABSTRACT: Low-density lipoproteins are the most common atherogenic particles in diabetic dyslipidemia; therefore statins, which dramatically reduce low-density lipoprotein (LDL) cholesterol, are first-line therapy for patients with diabetes. These agents produce equivalent relative risk reductions in those with and without diabetes but confer greater absolute risk reduction because of the increased incidence of ischemic cardiovascular events in those with diabetes. The LDL cholesterol goal for patients with diabetes who do not have coronary heart disease is below 100 mg/dL. For secondary prevention, the goal is below 70 mg/dL. High-dose statin therapy may be required to achieve these goals. Fibric acids are a reasonable initial option for patients with triglyceride levels above 200 mg/dL and high-density lipoprotein (HDL) cholesterol levels below 40 mg/dL; in such patients they reduce risk as effectively as statins. Intermediate-release niacin raises HDL cholesterol levels; the effect is enhanced when niacin is combined with a statin.
For 2 weeks, a 67-year-old obese woman has had episodes of diffuse, nonradiating abdominal pain that last for several hours and are slightly relieved by famotidine/antacid. She rates the pain as 7 on a scale of 1 to 10.
ROCKVILLE, Md. -- The FDA has approved lanreotide acetate (Somatuline) for the treatment of the rare endocrine disorder acromegaly.
MELBOURNE, Australia -- Adolescent boys deprived of a high glycemic index junk-food diet had better clearing of acne vulgaris in 12 weeks than a medicine chest full of pimple medications can provide.
NEW YORK -- Bone-generating osteoblasts secrete a protein that appears to regulate insulin function and glucose metabolism, revealing an endocrine role for the skeleton, researchers here said.
For several days, a 50-year-old man has had copious green stools, vomiting, and fever. His symptoms began shortly after he was discharged from a regional burn center, where he was treated for full-thickness burns that covered 60% of his body surface.
ABSTRACT: Angiotensin-converting enzyme inhibitors and ß-blockers are the cornerstone of heart failure medical therapy; unless contraindicated, start these agents as soon as possible after volume status has been optimized. Aldosterone receptor antagonists, angiotensin-receptor blockers, and a fixed-dose combination of hydralazine and isosorbide dinitrate (the last recommended especially for African Americans) can be used as add-on therapy. Prophylactic implantable cardioverter defibrillators reduce long-term mortality in symptomatic patients with a left ventricular ejection fraction (LVEF) of 35% or less. Cardiac resynchronization therapy improves symptoms and ventricular remodeling in some patients; indications include wide (more than 20 milliseconds) QRS complex on ECG, impaired LVEF (35% or less), and advanced heart failure symptoms (NYHA classes III and IV) despite optimal drug therapy. Measurement of natriuretic peptides and impedance cardiography both show promise for monitoring patients with heart failure and for guiding therapy, but definitive data to justify their routine use are still lacking.
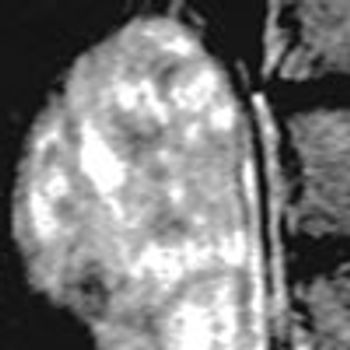
A large right adrenal mass was noted incidentally on an MRI scan of the lumbar spine, which had been performed for other reasons in a 55-year-old non-obese woman. The bright heterogeneous mass (T2-weighted image) measured 6.2 3 6.2 3 4.1 cm and sat like the head of a serpent on the superior pole of the right kidney. Its margins were smooth, but signal intensity was increased on T2 weighting because of high water content. The left adrenal gland was normal.
At a routine blood pressure check, a 63-year-old woman has 2 readings of 165/100 mm Hg. The patient has had essential hypertension since age 41 years. For more than a decade, it was easily controlled with a b-blocker; however, in recent years, her blood pressure has been more variable, with occasional readings of higher than 150/90 mm Hg.
CHICAGO -- A child who has a body mass index in the range of the 85th to 95th percentile for age and sex should be considered overweight, not "at risk of overweight".
SAN DIEGO -- Men older than 50 with androgen deficiency are at a greater risk for all-cause mortality than their peers with age-appropriate testosterone, reported investigators here.
To determine whether a midline neck swelling is caused by a thyroglossal cyst or by enlargement of the thyroid gland, ask the patient to open his or her mouth and move the tongue in and out.
ABSTRACT: Undiagnosed or persistent Helicobacter pylori infection and surreptitious or unrecognized NSAID use are the most common causes of refractory peptic ulcers. The use of antibiotics, bismuth, or proton pump inhibitors (PPIs) suppresses the H pylori bacterial load and may obscure the diagnosis. H pylori infections have also become more difficult to cure because of increased antibiotic resistance. For refractory infection, select an antibiotic based on in vitro susceptibility testing. When this is not available, combination therapy with a PPI, tetracycline, metronidazole, and bismuth is often effective. To detect surreptitious or inadvertent NSAID use, review the drug history in detail. When there is any doubt about such use, check platelet cyclooxygenase function.
Is it necessary to prescribe lipid-lowering therapy for a patient with a mildly elevated total cholesterol level (240 mg/dL), a low-density lipoprotein (LDL) cholesterol level of 120 mg/dL, and a high high-density lipoprotein (HDL) cholesterol level of 100 mg/dL?
Advertisement
Advertisement
Trending on Patient Care Online
1
Early Liver Disease Detection Starts in Primary Care: A Q&A With Stevan Gonzalez, MD
2
Retatrutide Achieved Up to 22.6% Weight Loss in 2 Phase 3 Obesity Trials
3
ACOG Releases New Guidance on HIV Screening and Prevention
4
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
5