




























































































































































During a routine skin examination, a papule of several years’ duration is noted on the upper lip of a 71-yearold man. The patient states that the lesion has been slowly enlarging; it does not bleed even during shaving.
During a routine skin examination, a papule of several years’ duration is noted on the upper lip of a 71-yearold man. The patient states that the lesion has been slowly enlarging; it does not bleed even during shaving.
We published a question from John Mosby, MD, who wanted to know why the zoster vaccine had been administered to an older man in an earlier Photoclinic case who had ophthalmic zoster. We also published the response from Dr Tran, which cited the Advisory Committee on Immunization Practices (ACIP) recommendation to administer the vaccine to all patients 60 years or older in whom it is not contraindicated, including those with a history of previous zoster.
A 5-year-old boy was brought for evaluation of left leg pain. He had awoken with the pain 2 days earlier.
A papular lesion developed rapidly during the previous 11 days on the left forearm of an 89-year-old man. Another patient noticed a similar growth that developed over a 3-week period on his finger.
This lesion looks suspiciously like a malignant melanoma.
A 60-year-old laboratory technician complained of a pruritic rash on and around her left ear. It had appeared a few days earlier, shortly after she cleaned her telephone receiver with a disinfectant. A tentative diagnosis of contact dermatitis was made, and treatment with a hydrocortisone cream was initiated.

A 14-year-old girl is seen because of long-standing nasal itch, intermittent nasal congestion, and clear nasal discharge. Allergies to house dust mites and to cats shown on prior skin testing. Often has marked eye swelling when exposed to cats. Receives antihistamines when in flare-up and prior to cat exposure. The consumption of dairy products exacerbates all of the above.

A 33-year-old woman presents with an asymptomatic facial rash for which she has been using mometasone cream regularly. Initially, she had a small patch of acne on one cheek that quickly cleared with this cream. However, the rash has been worsening for the past year.

For several months, a 51-year-old African American woman has had an asymptomatic erythematous papule on the nose. She is otherwise healthy.

These grouped, white to flesh-colored papules on the plantar aspect of a 28-year-old woman's heels appeared during weight bearing and disappeared in non–weight-bearing positions. The patient, a nurse whose work required standing for hours, noticed the lesions about a year earlier. Her medical history was unremarkable, and she was taking no medications. Her sister had similar lesions on her heels.

This rapidly growing red papule on the left palm of a 32-year-old man appeared a week after he underwent cryotherapy for wart removal. The patient denied any symptoms and had no significant medical history.
For several weeks, a 33-year-old man has had an asymptomatic lesion on the head of the penis. He has had a new sex partner in the past few months but is unaware of any health problems she may have. What is the likely cause of this lesion?

A 35-year-old man presents with a scaling rash on the penis of several weeks’ duration. Which of the following would you include in the differential?

Is this penile rash the result of lichen planus? Candidiasis? A dermatophyte infection? Seborrhea? Psoriasis? Click here for the answer.

For 2 months, a 27-year-old man has had this worsening rash on the head of the penis. He denies any history of trauma. What do you suspect?
A 74-year-old man with a history of diabetes mellitus, atrial fibrillation, and stroke had a stable, skin-colored mass on his upper back for the past 10 years that had suddenly become swollen and red.

During a skin cancer screening, a 45-year-old male soldier was noted to have bilateral subcutaneous nodules on the dorsa of his feet. The patient reported that the nodules had remained unchanged since they first appeared in his early 20s and were asymptomatic. He had no other lesions.
Physical changes that occur in aging skin (eg, dryness and thinning) can result in pruritus and cause patients to rub, scratch, and pick at their skin. These activities produce various dermatoses and reactive changes in the skin, such as postinflammatory pigmentary alteration. Lichen simplex chronicus (LSC) develops as a physiological cutaneous response to repetitive scratching or rubbing. First-line treatment consists of topical corticosteroids and application of ice to reduce the sensation of itching. Like LSC, prurigo nodularis results from rubbing and scratching the skin. Treatment is similar; however, intralesional corticosteroids and UV therapy play more of a role because prurigo nodularis is more intensely pruritic than LSC.
A hand mirror can aid in the examination of the legs and feet of a seated patient, such as one in a wheelchair. Use of a mirror obviates the need to “stand on your head” to visualize the soles, heels, and back of the legs. In addition, patients can be taught to use a mirror to examine their own feet and legs for skin breakdown or other pathological changes that herald potentially serious problems.
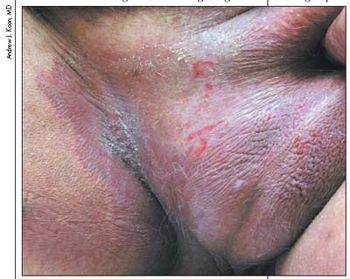
A 51-year-old man is seen because of a painful groin rash. Has not cleared despite 3 months’ topical corticosteroids and antifungals.

This rash on the face and neck of a 27-year-old man appeared periodically over a 2-month period. During this time, the patient’s work involved welding inside a steel oil tank. This photo was taken immediately after the patient had stopped working. He had no accompanying fever or respiratory symptoms. The urticaria was pruritic and resolved the following morning.
Having a magnifying mirror availablein each examination roommakes it easier for both patients andphysicians to identify facial lesions.

A 79-year-old man admitted for mental status changes, with neuroimaging that reveals lacunar brain infarct.
To avoid causing any exacerbation of a skin tear or similar wound when changing a self-adherent soft silicone foam dressing, I drawn an arrow on the dressing over the spot where the skin edges meet, running perpendicular to the skin flap. This minimizes the risk of recurrent trauma from raising the skin flap during dressing changes.

This dark maroon, cystic, dome-shaped, 8-mm lesion on a 75-year-old man’s back had been present for 2 years. It would occasionally bleed after minor trauma, such as when the patient dried his back with a bath towel. He had no history of skin cancer.