


























































































































































To ensure accurate joint injections, mark the site by firmly pressing the end of a closed ballpoint pen against the patient's skin.
Dermatology
Latest News
Advertisement
Advertisement
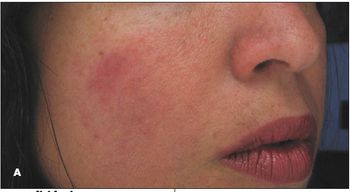
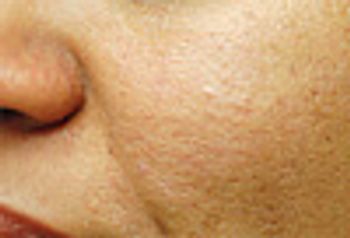
For several months, a 43-yearold woman had erythematous plaques on the cheeks that were more prominent on the right side. The patient had no pruritus but reported occasional facial burning. She had tried overthe- counter lotions but no medicated or corticosteroid topical preparations. She was otherwise healthy and was currently taking no medications.

This abdominal rash developed while a 63-year-old woman was traveling in Israel. She was admitted to the hospital, where she received intravenous antibiotics, and was discharged after 5 days. She now returns to the United States and wonders what she had, because she did not understand what the physician in Israel had told her. She has brought all of her medical records.

For 10 days, a 42-year-old woman has had this asymptomatic eruption on her trunk and proximal extremities. She is otherwise healthy.

A 63-year-old woman presents with a tender nodule of 10 days’ duration on the dorsum of her right hand. She does not remember any specific injury, but she does do her own housework. Another physician prescribed doxycycline, 100 mg bid; however, the nodule has persisted. You order a bacterial culture.

For 1 week, a 28-year-old man has had this tender, spreading rash on his chin. He is otherwise healthy. What does this look like to you?
A 72-year-old woman came to the emergency department with a tender, swollen left leg.

Several weeks earlier these slightly tender nodules erupted on the arms and legs of a 75-year-old woman with extensive sun damage.

An 80-year-old man presents for evaluation of highly pruritic blisters on the sides of his hands.

This rash on a 60-year-old man’s nose has worsened over the past few months.

This 39-year-old man from India has had an itchy eruption on his face for a few months. He is otherwise healthy, takes no medications, and has no other rashes.

A 24-year-old man was concerned about the small “bumps” on his abdomen that had been increasing in number over the past several years. They were asymptomatic. The patient denied a family history of similar lesions. Examination revealed about 15 to 20 scattered, nontender, skin-colored/bluish, firm 2 to 3-mm papules on the abdomen. No other cutaneous/mucosal findings were noted.
A 59-year-old man presented with painful paraparesis of acute onset, severe low back pain, and shortness of breath. On initial examination, he had 0/5 strength and numbness in his lower extremities. The skin from below his umbilicus to his lower legs was pale.

For 2 months, a 60-year-old man has had this pruritic eruption on his arms, legs, and trunk. It is itchy enough at times to interfere with his sleep. He has taken the same antihypertensive medication for more than a year.

This pruritic eruption appeared on the arms, thighs, and buttocks of a 28-year-old woman after the uneventful delivery of her second child.
Despite frequent application of lip balm, this split on a 46-year-old woman’s lower lip has failed to heal. What do you suspect?

A 46-year-old dentist presents for evaluation of chronic hand dermatitis of 1 year’s duration. He has no other rashes. Standard patch testing was negative. Another physician prescribed a high-potency corticosteroid cream that controls the rash but does not clear it. The patient takes no other medications.

At 1 week postpartum, a 32-year-old woman presents with an itchy rash of sudden onset. Famciclovir, 500 mg bid, is prescribed, but the rash persists.

This pruritic rash developed in a 43-year-old woman who had undergone a lumpectomy and lymph node dissection for breast cancer. She completed radiation therapy and chemotherapy 3 weeks ago. The rash has been present for 5 days. Levofloxacin was started 1 day ago.

A 24-year-old man seeks evaluation of a rash on his penis; it is associated with mild burning on urination. Workup for gonococcal and chlamydial infection is negative. He is otherwise healthy.
For the past month, a 39-year-old woman has had a persistent asymptomatic rash on her face. She is otherwise healthy and takes no medications.
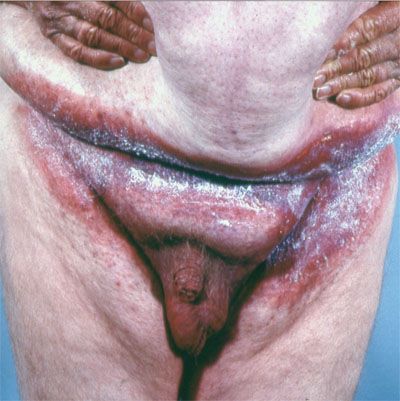
All elements of the skin are affected by age. In this 2-part article, I discuss how the blood vessels, the lymphatics, and the ground substance- which surrounds these vessels- respond to age, and I show how the aging elements of the vasculature can engender a variety of pathological cutaneous conditions.

This white patch in the medial periorbital area of a 15-year-old girl had been present for several months. It was asymptomatic. The patient denied having had an injury to the area. Results of a potassium hydroxide preparation of a skin smear and fungus culture were negative. She had no history of other hypopigmented lesions and was otherwise healthy. There was no family history of vitiligo or autoimmune disease.

For a few months, a 51-year-old woman has had an asymptomatic rash on her proximal thighs. She claims to have no other rashes and denies any exposure history.

The mother of a 10-year-old boy brings him for evaluation of a persistent rash on his shins of a few months’ duration. The rash has not responded to topical corticosteroids.
Advertisement
Advertisement
Trending on Patient Care Online
1
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
2
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
3
ACOG Releases New Guidance on HIV Screening and Prevention
4
Compulsive Smartphone Use Linked to Depressive Symptoms in Older Adults
5