

























































































































































A 51-year-old man presents with a painful inguinal rash that has persisted for 3 months despite application of a combination corticosteroid and antifungal cream. The rash is associated with a strong odor.
Obesity Medicine
Latest News
Advertisement
Advertisement
Urinary incontinence is common--especially among older adults--but underdiagnosed. Many persons with this disorder are reluctant to discuss it with their physicians; often, only direct questioning can uncover the problem.
57-year-old woman is hospitalized because of a 3-week history of persistent left-sided dull flank pain that worsens with movement and is associated with intermittent high fever.
Although proton pump inhibitors (PPIs) are highly effective, clinical failure in patients with gastroesophageal reflux disease (GERD) is seen regularly--not only in GI clinics but also in primary care offices. In fact, the prevalence of failure with PPIs has increased in proportion to the expanding indications for their use.

These yellow asymptomatic lesions on the inner upper eyelids of a 36-year-old woman had persisted for 2 years. She had a history of type 2 diabetes mellitus, migraine, nicotine dependence, bipolar disorder, and obesity. Her medications included quinapril, insulin aspart injection, sumatriptan, ziprasidone, and temazepam.
Scaling patches that resist antifungals; an outbreak of red papules; a velvety,hyperpigmented rash--can you identify the disorders pictured here?
A 51-year-old man with a 20-year history of asthma and seasonal allergies presented with low-grade fever, progressive dyspnea on exertion, and wheezing that had persisted for 2 weeks. Four days earlier, he had been seen by his primary care physician and had started levofloxacin therapy. However, his respiratory symptoms had worsened, warranting hospitalization. He also reported pain in the abdomen and left flank and pain and swelling in the right metacarpophalangeal and right shoulder joints.
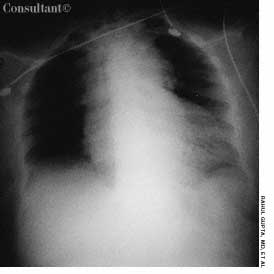
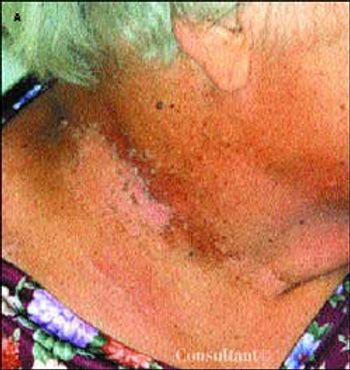
Abstract: Pleural tuberculosis and lymph node involvement are the most common extrapulmonary manifestations of tuberculosis. Most patients with pleural involvement complain of pleuritic chest pain, nonproductive cough, and dyspnea. The pleural effusion is usually unilateral and small to moderate in size. The diagnosis depends on the demonstration of acid-fast bacilli in pleural fluid or biopsy specimens, or the presence of caseous granulomas in the pleura. The gold standard for the diagnosis of lymph node tuberculosis is the identification of mycobacteria in smears on fine-needle aspiration cytopathology, histopathology, or mycobacterial culture. On ultrasonography and CT, the lymph nodes show enlargement with hypoechoic/hypodense areas that demonstrate central necrosis and peripheral rim enhancement or calcification. Treatment involves the combination of 4 antituberculosis drugs for 2 months, followed by 2-drug therapy for 4 months. (J Respir Dis. 2005;26(8):326-332)
What is the evidence that diet can reduce or increase the risk of common cancers? Is this evidence strong enough to warrant counseling patients to follow particular dietary guidelines?

A 62-year-old woman with a 25-year history of dyspnea was hospitalized because of hypoxemia. The dyspnea had become more severe during the past few years; it was worse in the standing position, was not exacerbated by walking, and was immediately relieved on lying down. She had no seasonal variation or environmental trigger of the dyspnea.
ABSTRACT: Early treatment with disease-modifying anti-rheumatic drugs (DMARDs)--alone or in combination-- can prevent joint damage and minimize disability. Until recently, the DMARDs used predominantly in patients with rheumatoid arthritis had been methotrexate, sulfasalazine, and hydoxychloroquine. Older DMARDs such as gold, d-penicillamine, and azathioprine have fallen out of favor because of their long- term toxicities or modest benefit. Six newer DMARDs--leflunomide, etanercept, infliximab, adalimumab, rituximab, and anakinra--have greatly expanded the current treatment options.
32-year-old man presents with a 4-day history of fever (temperature as high as 38.8 C to 39.4 C with severe rigors, chills, and profuse night sweats; generalized myalgias, including dull, aching headache; and dry cough.
The authors describe a rare cause of diffuse thoracic lymphadenopathy--Cogan syndrome. This case was remarkable for the temporal development of extensive lymphadenopathy independent of other hallmark symptoms and signs of this syndrome. In the appropriate clinical setting, Cogan syndrome should be considered in the differential diagnosis of thoracic lymphadenopathy.

During a routine annual checkup, a 5-ft 8-in, 94.5-kg (210-lb) 13-year-old girl was noted to have a hyperpigmented "dirty" lesion on the back of her neck. The girl's parents were also obese. Her mother had type 2 diabetes mellitus.
For several weeks, an 82-year-old woman had experienced blurred vision while reading. She was unable to localize the problem to either eye.
One third of all American adults (more than 70 million people) are currently on a diet. More than half of all adults have attempted dieting at some point--often more than once.
Abstract: Although excessive daytime sleepiness is most often simply the result of inadequate sleep, other causes must be considered as well. Common causes of daytime sleepiness include obstructive sleep apnea/hypopnea syndrome (OSAHS) and medication side effects. The differential diagnosis also includes narcolepsy and restless legs syndrome (RLS). In many cases, the answers to a few simple questions can provide the necessary clues to the diagnosis. Loud snoring is associated with OSAHS, while sudden muscle weakness triggered by intense emotion is consistent with narcolepsy. Referral for sleep evaluation is indicated to evaluate for OSAHS, narcolepsy, RLS, and idiopathic hypersomnia. Methods of measuring daytime sleepiness include the Multiple Sleep Latency Test and the Epworth Sleepiness Scale. (J Respir Dis. 2005;26(6):253-259)
Abstract: A number of scoring systems can be used to help predict difficult intubations. The Mallampati system, for example, can be useful in assessing patients before elective surgery, but it is less practical in emergent situations. Clinical features that suggest a potentially problematic airway include relatively long upper incisors, prominent overbite, narrow palate, edematous mandibular space, thick neck, and limited flexion of the neck. The most effective and rapid way of securing definitive airway management remains direct laryngoscopy with placement of an endotracheal tube (ETT). The ETT/stylet assembly of the light wand is best used when the patient can be successfully ventilated with a bag-valve mask device between intubation attempts. One of the most critical components of airway management is confirming that the ETT has been successfully placed in the trachea. (J Respir Dis. 2005;26(6):268-276)
A morbidly obese 63-year-old woman with type 2 diabetes mellitus and hypertension presented with postmenopausal vaginal bleeding. A uterine biopsy revealed papillary mucinous adenocarcinoma, and biopsy of a breast mass detected during the examination also showed adenocarcinoma. The patient underwent irradiation of the pelvis and breast.
Menstrual disorders are one of the most common complaints of women seen in primary care. Abnormal uterine bleeding (AUB) is a broad term that encompasses bleeding at abnormal or unexpected times or excessive flow at times of expected menses.
A 65-year-old woman with well-controlled hypertension comes in for a routine checkup. During the past 10 years, she has gained 25 lb and lost 1.5 inches in height.
As recommended by the authors, I commonly order a fasting lipid profile and measurements of glucose and insulin levels in children at risk for type 2 diabetes. One area of management that remains confusing is the approach to take with children who have an elevated fasting insulin level but otherwise normal laboratory results.
Several popular diets, such as the South Beach Diet and Sugar Busters, are based on the glycemic index; however, many patients are confused about its significance.
Primary care physicians are usually the first to see patients with joint pain; consequently they represent the "front line" of RA care. This fact-coupled with the projection that the number of rheumatologists is expected to decline by 20% during the next 2 to 3 decades-underscores the pivotal role that primary care clinicians are now expected to play in the early diagnosis of RA.
A 38-year-old man presented to the emergency department (ED) with a 2-week history of worsening shortness of breath and dry cough. He also complained of anorexia, a 14-kg (30-lb) weight loss over 3 months, pleuritic chest pain, and night sweats.
Advertisement
Advertisement
Trending on Patient Care Online
1
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
2
Newer GLP-1 Therapies Linked to Fewer Alcohol-Related Hospitalizations in Adults With AUD
3
Compulsive Smartphone Use Linked to Depressive Symptoms in Older Adults
4
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
5