

































































































































































ROCKVILLE, Md. - The FDA today approved Wellbutrin XL (bupropion extended release) for prevention of major depressive episodes in patients with a history of seasonal affective disorder (SAD). It is the first drug approved for SAD.
Obesity Medicine
Latest News

Advertisement
Advertisement
WASHINGTON ? Januvia (sitagliptin), an investigational oral agent for type 2 diabetes, appears to be effective when given as a monotherapy or as an adjunct to Glucophage (metformin) or Actos (pioglitazone), reported researchers here.
WASHINGTON ? Antidepressant medications appears to further increase the risk of developing type 2 diabetes in those with impaired glucose tolerance, researchers reported here.
WASHINGTON ? Preeclampsia is an independent risk marker for type 2 diabetes, even when gestational diabetes is taken into account, reported researchers here today.
ROCHESTER, Minn. ?Treating obese patients with chronic hepatitis C infection with a diet-and-exercise regimen could improve both their overall health and their response to antiviral therapies, researchers suggest.
A 22-year-old woman presents with fever and malaise of1 month’s duration. About 3 weeks earlier she went to theemergency department. Erythromycin was prescribed,and the patient was told to seek medical attention if hercondition did not improve. Since that time, her healthhas worsened, the fever has continued, and she has lostweight. She says she has had painful areas on her handsand feet but no rash.
Patients with psychiatric disordersoften present a diagnostic challenge-even for psychiatrists. Their demeanormay not readily reveal the nature orseverity of the problem. Nevertheless,there are clues that can help you sortthrough the differential and arrive atthe correct diagnosis.
The authors describe a woman who presented with severe pulmonary hypertension. A cardiopulmonary cause was initially sought, but thyrotoxicosis was the underlying cause.
Diabetic nephropathy, the leading cause of end-stage renal disease (ESRD) in the United States, affects 20% to 30% of patients with diabetes. Early diagnosis and aggressive treatment may delay the progression of kidney disease.
ABSTRACT: The key features of polycystic ovary syndrome (PCOS) are menstrual bleeding disturbances caused by chronic oligoovulation or anovulation and clinical or biochemical hyperandrogenism. The finding of polycystic ovaries on ultrasonography alone has limited predictive value. Obesity often coexists with PCOS and can exacerbate metabolic disturbances, particularly insulin resistance, but it is not a diagnostic finding. Laboratory results can rule out other conditions in the differential, such as an androgen- producing neoplasm, hypothyroidism, and late-onset congenital adrenal hyperplasia.
The secret to weight management is to communicate the answers to patients' questions about diet in a way that motivates them to apply the information. Here are some motivational strategies that may be effective.
The treatment of polycystic ovary syndrome (PCOS) is based on the patient's presenting symptoms and any significant abnormal findings. Symptoms can be managed with combined oral contraceptives (OCs), insulin-sensitizing agents, antiandrogens, and medications used to induce ovulation.
A long list of foodstuffs have been blamed for the nation's increasingly widespread weight and health problems. Now the spotlight has been turned not on what Americans eat--but on what they drink.
A 68-year-old man presented with diplopia, progressive dyspnea, leg swelling, weakness, night sweats, and a 9-kg (20-lb) weight loss. He had been healthy up until 2 weeks earlier, when the symptoms started. The patient's medical, social, and family history was noncontributory.
BOSTON - Symptoms of gastroesophageal reflux disease increase progressively with increasing body mass indices, even among normal-weight women, according to data from the Nurses' Health Study.
PAWTUCKET, R.I. - Patients may not be getting the message about the heart risks associated with dyslipidemia when the message is delivered by-the-numbers, according to researchers here.
My 46-year-old patient had a fasting plasma glucose level of 115 mg/dL; a followupfasting plasma glucose level was 116 mg/dL.
A 52-year-old man complains of right knee pain that hasbeen increasing steadily for several weeks. Two years earlierhe underwent a total arthroplasty of the same knee to treatsevere osteoarthritis secondary to a meniscal injury. He hasno history of recent trauma or increased activity.
Diabetes is epidemic! The numbersare truly alarming. In 1997, official datashowed that 16 million people in theUnited States had diabetes. Approximately1 million had type 1 disease,and 10.4 million had type 2 disease; theremainder had undiagnosed diabetes.1If these numbers are projected outagainst an annual increase in diseaseprevalence of about 3.5%, it means thatby the year 2028, 50 million people willhave diabetes. However, the actual rateis closer to 7% each year. As such, approximately100 million Americans-roughly 1 of every 4-will have diabetesby 2028.
Abstract: Exercise intolerance is common in persons with chronic obstructive pulmonary disease and can result from multiple physiologic factors, including dynamic hyperinflation, gas exchange abnormalities, and pulmonary hypertension. In the initial assessment, keep in mind that many patients underestimate the degree of their impairment. The 6-minute walk test is very useful in assessing the degree of exercise intolerance; when more extensive assessment is indicated, cardiopulmonary exercise testing (CPET) is the gold standard. CPET is particularly useful for defining the underlying physiology of exercise limitation and may reveal other causes of dyspnea, such as myocardial ischemia or pulmonary hypertension. Strategies for improving exercise tolerance range from the use of bronchodilators and supplemental oxygen to participation in a pulmonary rehabilitation program. (J Respir Dis. 2006;27(5):208-218)
Abstract: The management options for persons with obstructive sleep apnea-hypopnea syndrome (OSAHS) include lifestyle changes, continuous positive airway pressure (CPAP), oral appliances, and surgery. Lifestyle modifications work best in persons with mild OSAHS and may include weight loss and cultivation of good sleep habits, such as not sleeping supine. Before initiating CPAP therapy, polysomnography is recommended to determine the best airway pressure for the patient. Although the benefits of CPAP have been well documented, compliance remains an issue; some difficulties may be alleviated through patient/partner education and close follow-up. Oral appliances, which work by mechanically enlarging or stabilizing the upper airway, are preferred by some patients; however, they are less effective than CPAP at reducing the apnea-hypopnea index. Surgical interventions to alleviate upper airway obstruction can be used in select patients. (J Respir Dis. 2006;27(5):222-227)
An examination of the evidence on the cardioprotective benefits associated with various intensity levels, types, and amounts of physical activity, as well as tips on a beneficial yet realistic exercise program.
What factors are causing the increased incidence of hypertension and cardiovascular mortality in African Americans, and what can be done to counteract them?
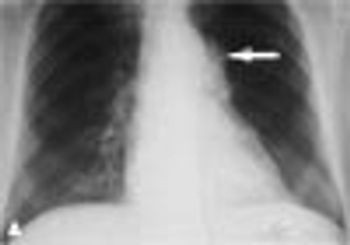
A 57-year-old woman presents with severe chest pain, and a frontal upright radiograph of the chest is obtained. What does this image reveal, and how will you arrive at a diagnosis?

A 62-year-old woman complained of right knee pain that had developed 1 year earlier after she had slipped on ice and fallen on the knee. Initial radiographs of the knee had shown mild degenerative changes. Treatment with NSAIDs for 10 months had failed to alleviate the pain.
Advertisement
Advertisement