





































































































































































To distinguish between hypertensive emergencies and urgencies and nonurgent acute blood pressure elevation, evaluate the patient for evidence of target organ damage. Perform a neurologic examination that includes an assessment of mental status; any changes suggest hypertensive encephalopathy. Funduscopy can detect papilledema, hemorrhages, and exudates; an ECG can reveal evidence of cardiac ischemia. Order urinalysis and measure serum creatinine level to evaluate for kidney disease. The possible causes of a hypertensive emergency include essential hypertension; renal parenchymal or renovascular disease; use of various illegal, prescription, or OTC drugs; CNS disorders; preeclampsia or eclampsia; and endocrine disorders. A hypertensive emergency requires immediate blood pressure reduction (although not necessarily to the reference range) with parenteral antibiotics. An urgency is treated with combination oral antihypertensive therapy.
Obesity Medicine
Latest News
Millions of Americans suffer from anxiety disorders. Many with panic disorder, social anxiety disorder, and/or generalized anxiety disorder present initially to their primary care clinician. Effective treatment is possible in a busy primary care setting; therapy involves patient education and pharmacotherapy. Once other potential causes of symptoms of an anxiety disorder have been ruled out, the first step is to reassure the patient that he or she has a psychological condition-a very common one-and that symptoms are not the result of an undiagnosed disease or "going crazy" or "losing control." Educate and inform patients that complete clinical remission is achievable, often with medication alone. Begin treatment on day 1 with a long-acting benzodiazepine-such as alprazolam XR or clonazepam-or with the anxiolytic agent buspirone; at the same time, start a selective serotonin reuptake inhibitor (SSRI). The anxiolytic agent allays acute somatic symptoms until the full effects of the SSRI are manifest (often 4 to 6 weeks). The anxiolytic can then be gradually tapered. Referral to a psychiatrist for psychotherapy may be indicated when a patient refuses or cannot tolerate drug therapy, or when response to therapy is inadequate.
ABSTRACT: The basic screening studies for rheumatic diseases are a complete blood cell count, a determination of the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) level, a rheumatoid factor assay, an antinuclear antibody (ANA) test, a measurement of serum uric acid level, and a urinalysis. Test results must be interpreted within a clinical context; for example, a positive ANA assay suggests the possibility of a rheumatic disorder, but it is not specific for any diagnosis. Tests that reveal the nature and extent of target-organ involvement, such as renal function studies in patients with systemic lupus erythematosus, can help guide the selection of therapy. Laboratory results also reflect disease activity; the ESR and CRP level are useful gauges of the activity of most inflammatory rheumatic disorders. Finally, laboratory monitoring can help you minimize the significant toxicity associated with many of the drugs used to manage rheumatic diseases.

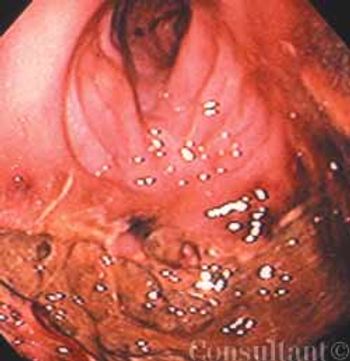
A52-year-old white man presented with a pruritic eruption on the neck of 3 months’ duration. The rash had not responded to a potent topical corticosteroid prescribed by another practitioner for the presumed diagnosis of eczema. The patient reported no current health problems. His history included a pubic louse infestation and several episodes of uncomplicated urethral gonorrhea. He readily admitted to having unprotected sexual intercourse with prostitutes.
Treatment of fibromyalgia syndrome (FMS) is a challenge. However, most patients benefit from appropriate management. Essential to treatment are a physician's positive and empathetic attitude, continuous psychological support, patient education, patience, and a willingness to guide patients to do their part in management. Other important aspects involve addressing aggravating factors (eg, poor sleep, physical deconditioning, emotional distress) and employing various nonpharmacologic modalities (eg, regular physical exercise) and pharmacologic therapies. Drug treatment includes use of tricyclic medications alone or in combination with a selective serotonin reuptake inhibitor, and other centrally acting medications. Tender point injection is useful. It is important to individualize treatment. Management of FMS is both a science and an art.
A 67-year-old Hispanic woman is seen for routine physical examination. Has mild hypertension but no other known medical problems. Feels well. No weight loss. No reported difficulty with eating, speaking, or swallowing. Denies any discomfiture in the mouth. States that nothing has changed in her mouth “ever since I lost my baby teeth.” Does not smoke cigarettes nor drink alcohol.
Is hypertension a frequent manifestation of thyroid disease?Which clinical clues suggest hypertension in persons with thyroiddysfunction?
Sudden profound vision loss in her left eye prompted an82-year-old woman to seek evaluation. She also complainedof “just not feeling well” and reported new-onsettemporal and occipital headaches of 6 weeks’ duration.
Signs and symptoms that strongly suggest peripheral arterial occlusive disease include diminished or absent pedal pulses, a unilaterally cool limb, and atrophic skin that is shiny and hairless. An ankle-brachial index of less than 0.5 suggests multisegment disease. Management goals are to decrease functional impairment, treat underlying atherosclerosis, and control risk factors. Smoking cessation is imperative. A graduated walking program is a mainstay of treatment and is associated with greater improvement in pain-free walking than is drug therapy. Surgery and percutaneous intervention are generally reserved for patients with lifestyle-limiting claudication, ischemic pain at rest, tissue loss, or gangrene.
A 75-year-old obese woman with subacute-onset dyspnea and lower right posterior chest pain was brought to the emergency department. She had a history of diastolic heart failure, arthritis, and suspected obstructive sleep apnea. The patient was dyspneic at rest.
ABSTRACT: The results of diagnostic tests do not correlate well with the presence and severity of pain. To avoid missing a serious underlying condition, look for "red flags," such as unexplained weight loss or acute bladder or bowel function changes in a patient with low back pain. Nonopioid medications can be more effective than opioids for certain types of pain (for example, antidepressants or anticonvulsants for neuropathic pain). When NSAIDs are indicated, cyclooxygenase-2 inhibitors are better choices for patients who are at risk for GI problems or who are receiving anticoagulants. However, if nonspecific NSAIDs are not contraindicated, consider using these far less expensive agents. The tricyclic antidepressants are more effective as analgesics than selective serotonin reuptake inhibitors. When opioids are indicated, start with less potent agents (tramadol, codeine, oxycodone, hydrocodone) and then progress to stronger ones (hydromorphone, fentanyl, methadone, morphine) if needed.

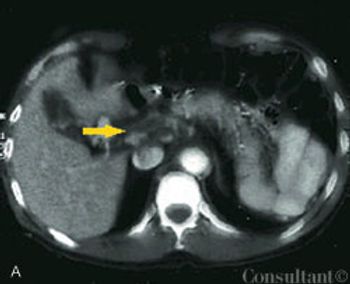
A 74-year-old woman was admitted to the hospital with abdominal pain, weight loss, fatigue, and change in bowel habits of 6 months’ duration. Her hemoglobin level was 7 g/dL; carcinoembryonic antigen, 672 ng/dL.
Uncontrolled hypertension is a major health problem among African Americans. Obesity, high sodium and low potassium intake, and inadequate physical activity have been identified as barriers to cardiovascular health in many African Americans. Thus, it is important to educate and counsel patients about lifestyle modifications, such as a low-sodium, DASH (Dietary Approaches to Stop Hypertension)-type diet; regular aerobic exercise; moderation of alcohol consumption; and smoking cessation. All classes of antihypertensive agents lower blood pressure in African Americans, although some may be less effective than others when used as monotherapy. Most patients require combination therapy. Both patient barriers (such as lack of access to health care and perceptions about health and the need for therapy) and physician barriers (such as poor communication styles) contribute to the low rates of hypertension control in African Americans. Patient-centered communication strategies can help overcome these barriers and can improve compliance and outcomes. Such strategies include the use of open-ended questions, active listening, patient education and counseling, and encouragement of patient participation in decision making.

A 62-year-old obese woman with adult-onset type 1 diabetes mellitus had a 6-year history of bilateral leg edema. During the last year, the edema worsened and the skin on her legs thickened. She also had multiple, bilateral, painful, superficial ulcers that drained copiously.
A 12-year-old African American girl comes to youroffice for a well-child checkup. She is tall for herage (height above the 95th percentile) and obese(body mass index [BMI] above the 95th percentile).Physical examination reveals acanthosisnigricans on her neck, axilla, and upper abdominalregion (Figure) and a vaginal yeast infection.Routine urinalysis reveals a glucose level ofgreater than 1000 mg/dL, with negative proteinand ketones. A random blood glucose test, obtainedbecause of the glucosuria, is 249 mg/dL.
An obese 55-year-old woman had intermittent dysuria and frequent urination for 4 days and fever, abdominal pain, and vomiting for 3 days. Her history included type 1 diabetes mellitus, hypertension, and angina; her medications included insulin, nifedipine, and nitroglycerin.
Persons with a systolic blood pressure (BP) of 120 to 139 mm Hg or a diastolic BP of 80 to 89 mm Hg are now considered, according to the latest Joint National Committee (JNC) report on hypertension.
ABSTRACT: When a patient presents with low back pain, ask about the location and quality of the pain, what makes the pain increase or decrease, associated symptoms, and risk factors. Clues to systemic causes of low back pain include fever; arthritis; iritis; signs and/or symptoms of GI disease, pelvic disease, or renal disease; tachycardia; and integumentary abnormalities. Perform a neurovascular evaluation as well as a detailed musculoskeletal examination. Imaging studies are not necessary for most patients initially. Acute therapy consists of the application of cold and heat and analgesics such as acetaminophen or an NSAID. Early exercise-not bed rest-is the cornerstone of treatment. Follow-up is mandatory: in 3 to 7 days for patients with severe pain, inconsistent findings, mild neurologic abnormalities, or a history of progres- sive symptoms; and in 10 to 14 days for patients with no neurologic compromise.
ABSTRACT: Indications for pulmonary function tests (PFTs) have widened substantially, ranging from screening smokers for early lung disease to determining the diagnosis and prognosis of pulmonary conditions. Current indications also include screening for drug-induced lung toxicity and preoperative screening for lung resection surgery. In the workup of respiratory symptoms, such as dyspnea, cough, and wheezing, PFTs can identify obstructive or restrictive patterns that may suggest a diagnosis such as asthma or interstitial lung disease. The ratio of FEV1 to forced vital capacity is very sensitive to the presence of airflow limitation, although bronchoprovocation testing may be needed to diagnose asthma, especially in patients with mild intermittent disease. Measurements of lung volumes and carbon monoxide-diffusing capacity (DLCO) provide crucial information in selected patients. For example, a reduced DLCO may be a sign of more advanced disease, such as emphysema or pulmonary hypertension.Since the first description of the spirometer by John Hutchinson in the late 1800s, pulmonary function tests (PFTs) have expanded to include spirometry; lung volumes; carbon monoxide-diffusing capacity (DLCO) (transfer factor); respiratory muscle performance; and exercise and functional testing, such as the 6-minute walk test (6MWT) and cardiopulmonary exercise testing (CPET).
The Geriatric Depression Scale is the most widelyvalidated screening tool. The questionnaire has beenreduced to a single question that is as sensitive and as specificas the 15-item shortened form of the original 30-itemscale. The question is: "How often do you feel sad or depressed?'This is certainly something that is easy to ask inthe course of a general physical examination or routine officevisit.
A 60-year-old man presented to the emergency department (ED) with fever of 1 day’s duration and midabdominal pain. The cramping pain had begun 3 days earlier in a bandlike distribution around the upper abdomen. Ingestion of food exacerbated the discomfort. The patient had a history of intermittent constipation; he denied alcohol or illicit drug use, nausea, vomiting, and weight loss. He did not use any herbal or over-the-counter medications.
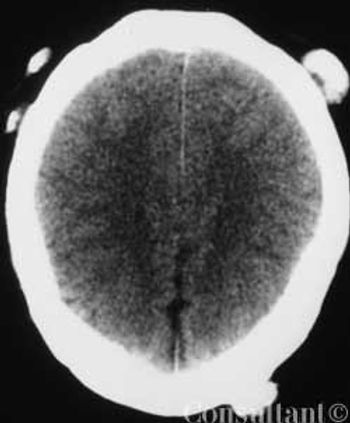
An otherwise healthy 38-year-old woman presented to the emergency department with a 1-day history of generalized left-sided weakness. She had no other significant medical history and was taking no medications. The patient was overweight.
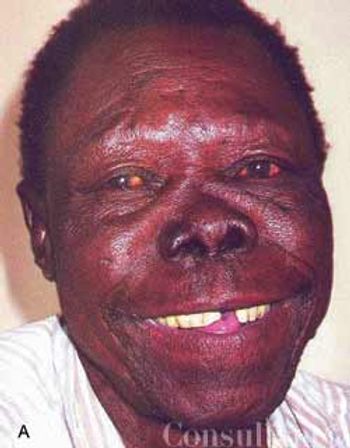
Leprosy, or Hansen disease, had recently been diagnosed in a 39-year-old man. He presented to the tropical disease unit of Harare Hospital, Zimbabwe, for follow-up.

Excessive belching, abdominal bloating, and flatulence caused an 89-year-old woman to seek medical attention. She reported that these previously mild and intermittent symptoms of 20 years’ duration had worsened during the last 2 years.
Persons with severe mental illnesses (SMI), such as schizophrenia, are at increased risk for comorbid conditions- including type 2 diabetes-independent of therapy. SMI sufferers especially at risk for type 2 diabetes are women, African Americans, and persons older than 45 years. Among the possible causes of increased susceptibility to type 2 diabetes are such schizophrenia-associated conditions as impaired glucose tolerance, overweight, obesity, inadequate nutrition, lack of exercise, and inadequate self-care. Other obstacles to good health care among patients with schizophrenia include impaired communication ability, denial of illness, social withdrawal, and undertreatment because of comorbid conditions. Different antipsychotic medications may also contribute to preexisting insulin resistance or glucose intolerance. Clinicians can optimize care by understanding the most significant barriers for each patient and incorporating this knowledge into an active treatment plan.