



























































































































































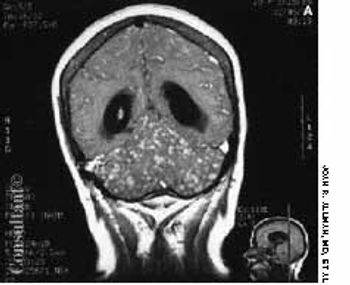
Fever of 1 month's duration was this 28-year-old man's only complaint. He had smoked marijuana in the past but denied intravenous drug use. His temperature was 39.4°C (103°F), but no other abnormalities were noted on physical examination.
Fever of 1 month's duration was this 28-year-old man's only complaint. He had smoked marijuana in the past but denied intravenous drug use. His temperature was 39.4°C (103°F), but no other abnormalities were noted on physical examination.

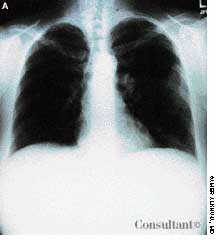
A 25-year-old man, who was an injection drug user, presented with a several-day history of dyspnea and fever. He complained of excessive malaise, fatigue, and weight loss but denied any hemoptysis. The examination of the lung revealed bilateral crackles in both lower zones.

A 43-year-old woman was hospitalized with a 3-day history of fever and back pain. She was malnourished and seropositive for HIV infection. Results of blood and sputum cultures were negative. A community-acquired pneumonia was diagnosed. Chest film findings and the clinical presentation were inconsistent with Pneumocystis carinii pneumonia.

Cough, fever, diarrhea, and weight loss had disturbed a 52-year-old woman for 1 month. AIDS had been diagnosed 5 years earlier, but she had declined medical treatment. The patient's vital signs were stable when she was admitted to the hospital. Physical examination results were unremarkable except for thrush and mild, diffuse abdominal tenderness.

A 2-week history of diarrhea mixed with bright red blood was the presenting complaint of a 40-year-old man who was seropositive for HIV. Stool studies and culture results were negative for microorganisms. Colonoscopy demonstrated only the raised vascular lesion seen here in the sigmoid colon, which may have been responsible for the bleeding.

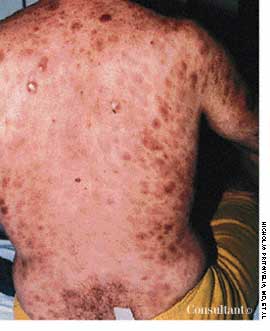
Purplish skin lesions appeared on the back and trunk of a 34-year-old homosexual man with HIV-1 disease. The spots had been growing larger over the past several weeks.
A 33-year-old man with AIDS presented to the emergency department with fever, dyspnea, cough, and pleuritic chest pain of 3 days' duration. He had had a Pneumocystis carinii infection 3 years before recently emigrating from the Dominican Republic to the United States. Promiscuous sexual activity was his only risk factor for HIV infection. The patient did not take antiretroviral medications or protease inhibitors because of their cost.
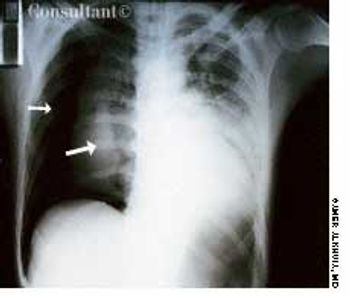
While watching TV, a 32-year-old man experienced acute right-sided pleuritic pain and was taken to the emergency department. He was seropositive for HIV but had never had Pneumocystis carinii pneumonia (PCP) and was not taking aerosolized pentamidine. Physical examination revealed hyperresonance with significantly decreased breath sounds over the right hemithorax.

For 2 months, a 22-year-old uncircumcised man noticed an asymptomatic, erythematous, static lesion on the glans penis. He had applied an over-the-counter “jock-itch” ointment for 2 weeks but to no avail. The young man was otherwise healthy and denied having dysuria or a history of sexually transmitted disease.

Persistent, unremitting itch-which intensifies at night-is the chief complaint of patients with scabies. The female Sarcoptes scabiei mite (A) burrows into the stratum corneum, where she lays eggs. The parasite is transferred by intimate contact and fomites, such as infested clothing, towels, and bedding.

A painful swelling over the right lower eyelid with conjunctival injection was evaluated in a 28-year-old injection drug user. Cephalexin and corticosteroid ophthalmic drops failed to resolve the condition.
A comatose 29-year-old woman was brought to the emergency department. Her family reported that she had been well until 4 days earlier, when headache and fever developed. She went to another hospital at that time and was told she had an abscessed tooth. She was given erythromycin, and the tooth was extracted the following day. The patient's headache and fever worsened; a sore throat also developed, and a rash appeared on her trunk, arms, and legs. The family denied any HIV risk factors, unusual medical history, recent travel, and exposure to persons with infectious diseases.
For the past 2 days, a 30-year-old man had experienced scant hemoptysis. He had also lost a significant amount of weight-5 kg (11 lb)-over the last 2 months. The patient, a recent emigrant from Ecuador, had no history of tuberculosis (TB) or of exposure to this disease, and he had not been skin tested with purified protein derivative (PPD). He denied exposure to risk factors for HIV infection.

An obese 52-year-old woman with a 5-year history of type II diabetes mellitus had odynophagia and dysphagia for several days. She described the sensation as food “sticking” in her chest. She also complained of vaginal itching, polyuria, and polydipsia. The only remarkable finding on physical examination was candidal vaginitis. The patient did not smoke cigarettes or drink alcoholic beverages, and there was no history of recent weight loss.

A previously healthy 51-year-old man presented with weight loss and poor appetite of 2 months' duration. He was heterosexual and had many sexual partners. Except for a temperature of 38.3°C (100.9°F) and left basal rhonchi, results of physical examination were normal. A chest radiograph and CT scan, as seen here, showed large cavitary lesions in the lower left lobe.
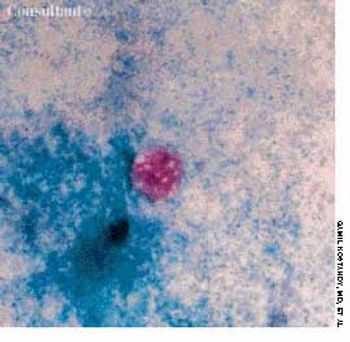
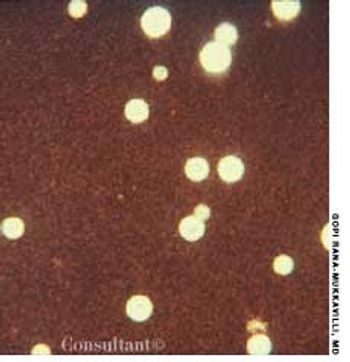
A 32-year-old Hispanic woman with AIDS presented with a 1-month history of diarrhea; abdominal bloating and cramps; loss of appetite; and pronounced fatigue, malaise, and weight loss. She had no fever or chills and was not vomiting. Her CD4+ cell count was 12/µL. Results of a routine microscopic examination of stool for ova and parasites were negative; an acid-fast stain of stool demonstrated oocytes of Cyclospora cayetanensis measuring 8.8 mm in diameter (pictured, magnification ×1,000). This is about twice the size of the Cryptosporidium parvum oocyte, which typically is 4 to 5 mm.
Fever occurring twice daily, accompanied by profuse sweating, anorexia, and malaise of 15 days' duration resulted in hospitalization of a 31-year-old woman. At this time, her temperature was 37.6°C (99.7°F); blood pressure, 110/70 mm Hg; pulse rate, 90 beats per minute; and respiratory rate, 18 breaths per minute. A palpable spleen was about 3 to 5 cm below the left subcostal margin. Neither lymphadenopathy nor hepatomegaly was noted.

The widespread eruption of asymptomatic macules and flat, palpable, flesh-colored lesions prompted a 23-year-old woman to consult her physician. The lesions-some of which had dark centers-were concentrated on the patient's face, neck, and upper back; the palms, soles, anal mucosa, and genital areas were clear. The patient denied systemic symptoms. She was seronegative for HIV.

A 52-year-old white man presented with a pruritic eruption on the neck of 3 months' duration. The rash had not responded to a potent topical corticosteroid prescribed by another practitioner for the presumed diagnosis of eczema.

Severe shortness of breath, a dry cough, and a 10-day history of fever sent a 37-year-old man with HIV disease to the emergency department. He complained of a poor appetite and had lost 10 lb over the last 10 days.

During the past 2 weeks, a 34-year-old man with HIV infection experienced worsening mouth pain while chewing.

A 29-year-old man presented with a complaint of venereal warts and a long history of mild psoriasis, which he had treated with fluocinolone. He returned 3 months later complaining of chest congestion of 10 days' duration; it had been treated with ciprofloxacin at an urgent care facility.
A 48-year-old man with jaundice, nausea, vomiting, and abdominal pain was hospitalized. The patient-a recovering alcoholic-was afebrile and reported abstinence from alcohol for 6 months.

For the past 3 months, a 66-year-old man has suffered fatigue and loss of appetite and weight. He was not coughing, nor had he experienced fever, chest pain, or hemoptysis. He had no history of notable respiratory disease, and he was not aware of having had tuberculosis (TB).

After 1 day of upper abdominal pain, nausea, and vomiting, a 32-year-old man sought medical care. He had no significant medical history. The patient had tenderness and guarding in the right upper quadrant; no mass was detected. The remainder of the physical examination was normal.