




























































































































































ABSTRACT: The interpretation of acid-base data can be greatly facilitated by applying 5 rules: (1) use the arterial pH to detect acidemia or alkalemia, (2) use the PCO2 and bicarbonate level to determine whether the underlying cause of acidemia or alkalemia is respiratory or metabolic, (3) calculate the anion gap to help identify the presence and nature of metabolic acidosis, (4) assess the degree of compensation, and (5) determine whether quantitative changes in the different groups of anions in the blood are in a 1:1 relationship. Rules 4 and 5 can help detect an occult acidosis or alkalosis. Use the osmol gap to identify the cause of an elevated anion gap metabolic acidosis. Non-anion gap metabolic acidosis results from bicarbonate wasting by either the gut or the kidney; measure urinary electrolytes and calculate the difference between positive and negative charges to determine which organ is responsible. Measure the urinary chloride concentration, blood pressure, and renin and aldosterone levels to detect the cause of metabolic alkalosis.
Hypertension
Latest News

Many patients who present to the emergency department(ED) with severe headache request a narcotic to relieve thepain.
A 54-year-old man is admitted to the hospital because of worsening lower extremityswelling and knee and ankle pain and stiffness. These symptoms havemade walking very difficult for the past month.
Recently, the National High Blood Pressure Education Program Coordinating Committee updated its 1993 recommendations for primary prevention of hypertension.
ABSTRACT: The most common errors in measuring blood pressure (BP) are using the incorrect cuff size, not having the patient relax for 5 minutes before the measurement, and deflating the cuff too quickly. Observer bias may compound technical errors. When patients use the proper procedure, home BP measurements may be more reproducible than office measurements. Brachial artery-based monitors are more accurate than finger- or wrist-based instruments. To ensure that patients measure their BP correctly, observe their technique with their own monitors. Counsel patients to measure their BP at predetermined times and to have their monitors validated periodically.
For the past several weeks, a 54-year-old man has had progressivelyworsening abdominal pain and general achiness.He has no nausea, vomiting, diarrhea, or fever and no historyof trauma.
A 76-year-old woman is admitted to the hospital for increasing fatigue and weaknessthat began about 3 weeks earlier. Her symptoms have worsened duringthe past week to the point of profound weakness and both dyspnea and nearsyncopewith minimal exertion.
In their case report, “Sudden Headache in a Woman With Hypertension” (CONSULTANT,July 2002, page 1049), Drs Gary Quick and Maggie Law describe apatient with uncharacteristically severe headache and very high blood pressure.
Cardiac stress imaging has become increasingly sophisticated; nevertheless, standard exercise electrocardiography can provide valuable clinical information, such as time to onset of angina or ST-segment depression, maximal heart rate and blood pressure response, and total exercise duration. Pharmacologic stress agents may be substituted for patients who cannot exercise on a treadmill; however, these agents must be used in conjunction with echocardiography or nuclear scintigraphy to obtain adequate diagnostic information.
A 53-year-old man has hadmalaise, intermittent cough, and occasionalfever and night sweats for 2weeks. He has also lost some weightduring this time but denies hemoptysisand sputum production; he hasnot traveled abroad recently. His onlysignificant medical condition is hypertension,which is well controlled withmedication.
Glaucoma isthe leadingcause ofblindness inthe UnitedStates.1Nearly 3 millionpersons have the disease,and about 100,000 newcases are diagnosed eachyear.1 Between 3 and 6 millionAmericans are thoughtto be at increased risk forglaucoma because of elevatedintraocular pressure(IOP).2
A 78-year-old man presented to theemergency department with a 3-weekhistory of progressive shortness of breathand cough with blood-streaked, yellowishsputum. The patient had dyspnea onexertion limited to 2 blocks, 2-pilloworthopnea, paroxysmal nocturnal dyspnea,and nocturia. Neither fever norchills were present. He had lost 7.2 kg(16 lb) during the last year.
A 69-year-old retired accountant presents with a 2-month history of daily headaches. The pain is moderate, constant,global, pressure-like, and occasionally pulsating; it is sometimes exacerbated when the patient lies down. He denies nauseaor vomiting, ocular symptoms, weakness, or sensitivity to light. His wife reports that years ago he experienced throbbingheadaches regularly.
During a routine office visit, a 64-year-old woman who has had type 2 diabetesfor more than 10 years complains of increased pedal edema. The edema is minimalon awakening and worsens throughout the day.
My patient is a 42-year-old woman who experienced a nonblanching, purpuricrash and edema of the lower legs after she started taking nifedipine (Figure).
A 72-year-old man sought medical evaluationafter he awoke and was unableto open his right eyelid (A). He deniedpain, recent trauma, and diplopia. Thispatient’s history included well-controlledhypertension and hypercholesterolemia,for which he was taking atorvastatin.He did not have diabetes.

For 2 days, a 68-year-old woman had watery, yellowish diarrhea with mucus and left lower quadrant pain. Her medical history included hypertension, diabetes mellitus, and congestive heart failure (CHF); she had left the hospital 5 days earlier following treatment of an exacerbation of CHF with intravenous furosemide and sodium and fluid restriction. The patient was taking furosemide, lisinopril, and glipizide; she denied any recent antibiotic therapy.

A 64-year-old woman with a history of diabetes, hypertension, and lymphoma was admitted to the hospital with a dull headache, conjunctival congestion, and slight dyspnea. Her pulse rate was 96 beats per minute; blood pressure, 146/68 mm Hg; and respiration rate, 22 breaths per minute. She also had increased jugular venous distention; cardiovascular and chest examination findings were normal. Edema of both arms and dilated blood vessels on the anterior chest wall were noted.
A 63-year-old woman seeks evaluation of a persistent, rough, red area onthe dorsum of her left index finger. The lesion has been present for severalmonths. The patient’s manicurist is convinced it is a wart.
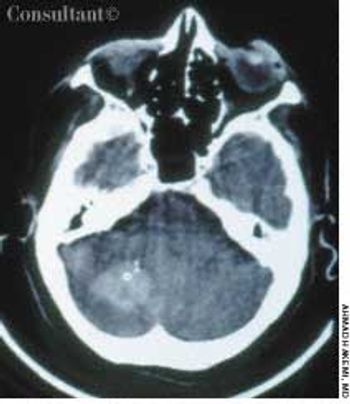
A 65-year-old woman with a long history of hypertension treated with metoprolol and felodipine complained of dizziness, headache, nausea, and vomiting of acute onset. Her blood pressure was 220/110 mm Hg. She was drowsy and unable to stand or walk.
Many of my older women patients think theyare at much higher risk for breast cancer thancoronary heart disease (CHD). How can we raise women'sawareness about their risks of CHD and therebyencourage them to take measures to prevent it?
Q:Should I avoid angiotensin-converting enzyme (ACE) inhibitors in mypatients with progressive renal insufficiency?
Q:Many of my patients appear to have white-coathypertension: their pressure is elevated whenmeasured in my office-but normal when measured athome. Am I ignoring significant hypertension if I do nottreat these patients? Or am I overtreating if I do treat?
A 37-year-old woman presents to the emergency departmentwith a diffuse, sharp, pounding headache,which started 2 hours earlier. She rates her discomfort as4 on a scale of 1 to 10. Neck muscle soreness is also present,but the pain does not radiate.

A 72-year-old woman presented for her annual physical examination. She had been treated for tuberculosis 20 years earlier. The patient did not smoke cigarettes; she denied fever, chills, and rigors.