



























































































































































In their "What's The 'Take Home'?" case of a pregnant woman with hypertension, Drs Lawrence Kaplan and Ronald Rubin inquire into the most likely cause of the patient's elevated blood pressure. However, this information is not sufficient to make a definitive diagnosis.
Hypertension
Latest News
Advertisement
Advertisement

An 83-year-old man with a history of hypertension and coronary artery disease presented with a 4-day history of mental status changes, slurred speech, and difficulty ambulating. He reported a lack of appetite and weakness of several days.
A serum alkaline phosphatase (ALP) level three times higher than normal, found on routine laboratory examination, prompted further evaluation of a 57-year-old man. At admission, his temperature was 36.8°C (98.2°F), blood pressure was 120/85 mm Hg, pulse rate was 90 beats per minute, and respiration rate was 19 breaths per minute. The physical examination was unrevealing, and the patient's personal and family medical histories were unremarkable.
A 62-year-old African American woman was brought to the emergency department (ED) after the sudden onset of slurred speech and weakness in her left arm and leg. Her medical history included hypertension, insulin-dependent diabetes, and congestive heart failure.

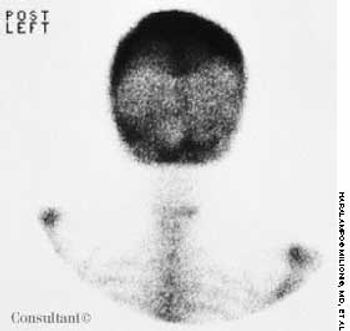
Frequent urinary tract infections and unexplained hypertension (160/100 mm Hg) occurred in a 38-year-old man with no significant medical history. The heart and chest were normal; a right lower quadrant mass was detected in the abdomen. Red blood cells were found in the urine. An abdominal CT scan demonstrated that the left kidney was fused to the lower pole of the right kidney with the left pelvicaliceal system to the left of the midline; these findings are consistent with crossed fused renal ectopia. Cystographic and cystoscopic examinations were normal.

A 35-year-old man, a smoker, had right pleuritic pain, productive cough, and fever for 3 days. His pulse rate was 107 beats per minute; respiratory rate, 14 breaths per minute; blood pressure, 136/80 mm Hg; and temperature, 37.7°C (99.9°F). There were signs of right upper lobe consolidation. Laboratory studies showed hyponatremia. Chest films showed a homogeneous density in the right upper lobe.

A 41-year-old man complaining of left-sided chest pain for 2 hours was examined in the emergency department (ED). On arrival, his blood pressure was 160/100 mm Hg; heart rate, 90 beats per minute; respiratory rate, 18 breaths per minute; oxygen saturation, 99%; and temperature, 37.2°C (99°F).

Police brought a delirious, combative 24-year-old man to the emergency department. The patient was unable to provide any history on arrival, but his scarred, blistering lips and his vital signs (blood pressure, 166/102 mm Hg; heart rate, 97 beats per minute; respiratory rate, 24 breaths per minute; and temperature, 38.2°C, or 100.9°F) led to a possible diagnosis of cocaine-induced delirium.

An 80-year-old woman presented with recurrent abdominal pain for 1 month, constipation, and vomiting. She had no diarrhea, rectal bleeding, or weight loss.

A 49-year-old woman with a history of alcoholic cirrhosis, esophageal varices, coronary artery disease, diabetes mellitus, and hypertension presented to the emergency department with a 2-day history of fever, chills, nausea, and back and abdominal pain. The pain began on the right side, progressed to the lower back, and radiated into the right anterior thigh and groin area.
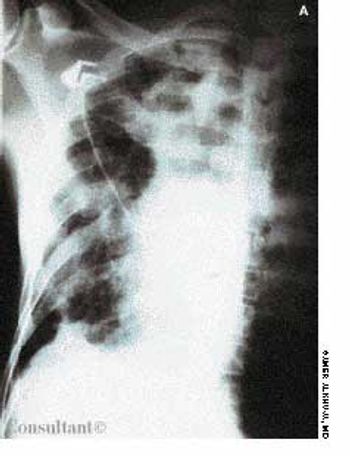
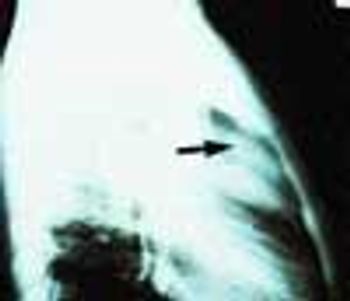
Presenting symptoms of this 42-year-old man were left pleuritic pain and severe dyspnea while climbing stairs. He had a 2-year history of exertional dyspnea but had not sought medical advice. The patient's pulse was 123 beats per minute; respiratory rate, 45 breaths per minute; blood pressure, 80/45 mm Hg; and temperature, 37.3°C (99.1°F). Chest examination revealed hyperresonance with absence of breath sounds over the left hemithorax and wheezing over the right lung.

Levofloxacin, 500 mg/d, had been prescribed for a 74-year-old woman who had a urinary tract infection. The patient had type 2 diabetes and hypertension. She was allergic to sulfa drugs.

A 73-year-old man was admitted to the hospital with pain in his hands, feet, and elbows. The patient, an alcoholic, had a 20-year history of hypertension and diabetes. Deformities of the hands and feet had developed during the past 5 years. Tophi were present over both ear lobes. The serum uric acid level was 15 mg/dL.
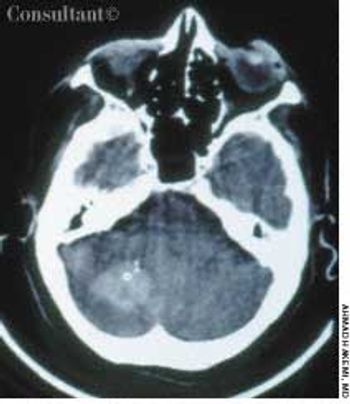
A 65-year-old woman with a long history of hypertension treated with metoprolol and felodipine complained of dizziness, headache, nausea, and vomiting of acute onset. Her blood pressure was 220/110 mm Hg. She was drowsy and unable to stand or walk.

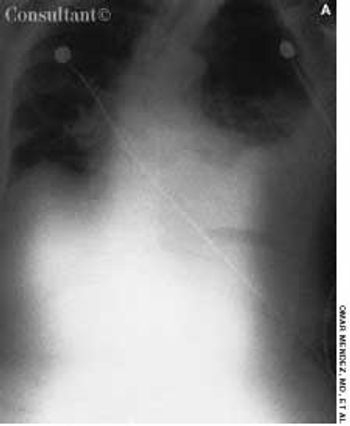
A 64-year-old woman with a history of diabetes, hypertension, and lymphoma was admitted to the hospital with a dull headache, conjunctival congestion, and slight dyspnea. Her pulse rate was 96 beats per minute; blood pressure, 146/68 mm Hg; and respiration rate, 22 breaths per minute. She also had increased jugular venous distention; cardiovascular and chest examination findings were normal. Edema of both arms and dilated blood vessels on the anterior chest wall were noted.
A 72-year-old woman who had fallen and injured the left side of her chest came to the emergency department complaining of pain in that area. She was physically stable and not short of breath. A soft systolic murmur was heard over the left precordium; the lungs were clear. A posteroanterior chest film showed no rib fracture but it did show an enlarged heart and a large, calcified ventricular aneurysm.

A 97-year-old woman with a history of hypertension and a paraesophageal hiatal hernia presented with abdominal distention and shortness of breath. Three days earlier, she had fallen and sustained a hairline pelvic fracture; she was evaluated in the emergency department and given narcotics for the pain. Subsequently, the patient's abdomen became increasingly distended, and she had no bowel movement for 3 days.

A 79-year-old nursing home resident was hospitalized for evaluation of hyperkalemia and leukocytosis. Her medical history included hypertension, respiratory failure with subsequent tracheostomy placement and ventilator dependency, and anemia. Both of her legs had been amputated above the knee secondary to complications of type 2 diabetes mellitus.
An 85-year-old white woman was brought to the emergency department (ED) with acute, severe left posterolateral chest wall pain of several hours' duration. The nonradiating pain was accompanied by shortness of breath. She denied palpitations, diaphoresis, syncope, or dizziness.
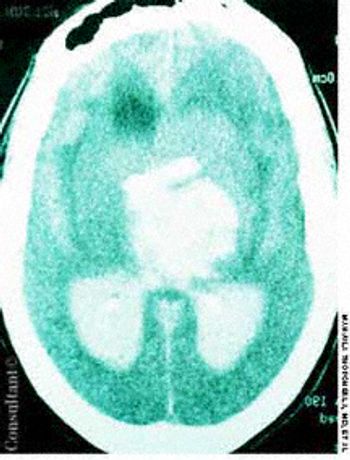
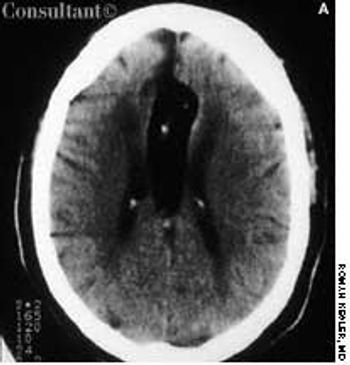
A 60-year-old comatose man was brought to the emergency department (ED). He had a history of diabetes, hypertension, and alcohol abuse. Relatives reported that the patient was noncompliant with his antihypertensive medication regimen.

A 46-year-old woman sought treatment of vaginal pruritus of 6 months' duration. She also was bothered by generalized skeletal aching that was most prominent in her legs. The patient had a history of hypertension.
Cirrhosis and ascites developed in a 52-year-old man with a history of chronic hepatitis C and ethanol abuse. He was hospitalized because of bleeding esophageal varices, which were successfully treated with elastic band ligation.
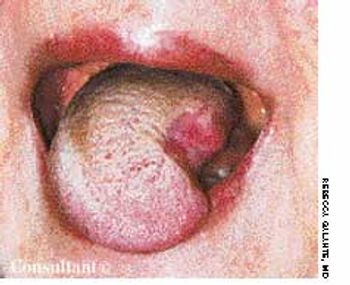
The initial complaint of a 79-year-old woman was of mild headache, neck pain, and sore throat. She had a history of hypertension, diabetes mellitus, and heavy cigarette smoking. Examination by an otolaryngologist, which included laryngoscopy, revealed no abnormalities. Three weeks later, the patient's throat and neck pain became more severe. She had no arthralgias, visual loss, fever, or worsening head pain.

The parents of a 10-year-old boy of normal intelligence brought him for evaluation because of his tall stature. He was 154 cm tall (3 cm above 97th percentile) and weighed 34.3 kg (50th percentile). He exhibited significant arachnodactyly, with an upper to lower segment ratio of 0.8 and an arm span to height ratio of 1.1. He had a long, angular face with a high arched palate and crowded dentition, ptosis, myopia, superior lens subluxation, pectus excavatum, widely spaced and low-set nipples, grade 2/6 ejection systolic murmur at the left sternal border, midthoracic scoliosis, joint hypermobility, positive thumb sign and wrist sign, and pes planus.

For 36 hours, a 75-year-old woman had experienced weakness of the right side of the face. She was unable to close the right eye and drooled from the right side of the mouth. There was no weakness, numbness, or tingling of the extremities. The patient's medications included insulin for type 2 diabetes, furosemide and spironolactone for hypertension, aspirin, alendronate, calcium, vitamin D, and tramadol for occasional pain from osteoarthritis.
Advertisement
Advertisement
Trending on Patient Care Online
1
ACOG Releases New Guidance on HIV Screening and Prevention
2
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
3
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
4
FDA Accepts Cefiderocol sNDA for Pediatric Gram-Negative Infections
5