


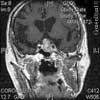



























































































































































The patient is a 47-year-old man who began to experiencefrequent headaches about 6 years before hepresented to a neurology clinic. The headaches rapidly progressedto become daily and almost constant. He describeda sensation of dull pressure in both temples that was presenton or within a few hours of awakening and that persistedfor the remainder of the day. He experienced a moreintense, disabling, throbbing pain in the same locationonce or twice a week, with photophobia and nausea, thatmight last 2 to 3 days. The patient took 2 to 6 over-thecounter(OTC) analgesic tablets each day-usually200 mg of ibuprofen. These would dull but not terminatethe pain.
Hypertension
Latest News
Advertisement
Advertisement
High-grade fever, chills, fatigue, malaise, and anorexia developed in a 35-year-old man following subclavian catheterization because of chronic renal failure of unknown cause. The patient, who had long-standing diabetes mellitus, was admitted to the ICU with the diagnosis of possible sepsis. The next day, he was found to have a grade 2/6 systolic murmur compatible with tricuspid regurgitation. This was confirmed when a 4-chamber echocardiogram (A) revealed a large single piece of vegetation (2 arrows) lying on the tricuspid valve, flapping in and out of the right ventricle. In a 2-dimensional echocardiogram of the right atrium and right ventricle (B), 3 arrows point to the vegetation. (RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium; TV, tricuspid valve.)
An 83-year-old woman is brought by her daughter for evaluation becauseof increasing confusion during the past few days. The patienthas early Alzheimer dementia, hypertension, and type 2 diabetes. She takes donepezil, 10 mg/d;lisinopril, 5 mg/d; and glipizide, 5 mg bid. She is unable to bathe and dress herself as well as previously,has been crying for no apparent reason, and has lost her appetite.
ABSTRACT: The prevalence of erectile dysfunction (ED) is higher among men with hypertension than among normotensive men. Sexual dysfunction is a common side effect of many antihypertensive medications and can lead to noncompliance. Treatment-related ED is more often associated with diuretics and ß-blockers and is less common with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers. If ED complicates therapy, consider switching to an antihypertensive agent with fewer sexual side effects. However, if compelling reasons exist for the use of a particular antihypertensive agent (eg, a ß-blocker in a patient with previous myocardial infarction), several options for the treatment of ED are available. Phosphodiesterase-5 inhibitors have been shown to be safe and effective in men who are receiving antihypertensive therapy.
ABSTRACT: The early signs of diabetic neuropathy can be detected during a routine clinical examination. Inspect patients' feet for deformities and sensory loss, which indicate risk of ulceration. Prolonged poor glycemic control, alcohol abuse, and obesity increase the risk of amputation. Autonomic dysfunction, which can lead to sexual dysfunction and gastropathy, can be detected by measurement of heart rate and blood pressure. A resting heart rate of about 100 beats per minute and a decrease of about 30 mm Hg in systolic blood pressure within 2 minutes of standing are abnormal findings. Electromyography and nerve conduction studies confirm the diagnosis. Improved metabolic control is the main goal of treatment. Analgesics, neuromodulators, and tricyclic antidepressants are effective for managing pain. In patients with autonomic neuropathy, treat the associated symptoms.
A 20-year-old woman presents with a 3-week history of a pruritic, progressivelyenlarging erythematous lesion on one arm. She has a cat and recentlystarted horseback riding lessons. She is otherwise healthy and takes nomedication.

A 53-year-old man with type 2 diabetes mellitus and hypertension presented to the emergency department with pain in his left upper chest and back, neck, and shoulder. The pain increased with passive and active range of motion testing and decreased at rest. His physical examination was unremarkable except for restricted left shoulder movement and generalized tenderness in the left shoulder area.
ABSTRACT: The Studies of Left Ventricular Dysfunction (SOLVD) trials demonstrated that early intervention in congestive heart failure (CHF) improves survival. However, early CHF is mainly a clinical diagnosis based on New York Heart Association criteria and, until recently, no easy and inexpensive screening test existed. There are now several such tests that employ radioimmunoassays (RIAs) to measure cardiac peptides in a single plasma sample; results help determine the likelihood that CHF is present but do not definitively establish the diagnosis. The vessel dilator RIA is the most specific and sensitive for differentiating persons with mild CHF from healthy ones; intravenous administration of this cardiac peptide hormone has beneficial hemodynamic, diuretic, and natriuretic properties in persons who have CHF. Brain natriuretic peptide (BNP) measured by fluorescence immunoassay is useful in the emergency department, because a result may be obtained in as little as 15 minutes. This assay may indicate CHF; further tests are recommended to define the diagnosis. BNP increases with other causes of dyspnea, including pulmonary hypertension, pulmonary emboli, and renal failure, so it is not specific for CHF. BNP also increases with age, and measured values are higher in women than in men.
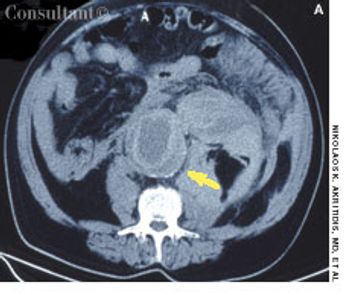
A 30-year-old man presentedwith severe left flankpain radiating to his abdomenand gross hematuriaof 5 to 10 days’ duration.He also reported a 4- to 6-monthhistory of nausea with intermittentvomiting, anorexia, and progressiveweight loss. He took no medicationsand had no allergies.
A 60-year-old woman with hypertension, diabetes mellitus, and intermittentatrial fibrillation presents with nausea, diaphoresis, dizziness, and globalweakness that has lasted 1 hour. She denies chest pain, dyspnea, syncope,vomiting, diarrhea, blood loss, and headache; there is no vertigo. Medicationsinclude acetaminophen, digoxin, diltiazem, glipizide, hydrochlorothiazide,irbesartan, metformin, pioglitazone, and warfarin.
A 48-year-old woman with a historyof hypertension and mildasthma has been transferred to themedical service because of an abnormalpostoperative ECG. She hadbeen admitted 2 weeks earlier to thegynecology-oncology service for localrecurrence of a previously resecteduterine sarcoma and underwent laparotomyfor debulking of the pelvicmass and resection of the rectosigmoidcolon. She did well until postoperativeday 14, when sudden chestpain and dyspnea developed.
ABSTRACT: Guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction have been updated following results from pivotal controlled trials. The new American College of Cardiology/American Heart Association guidelines stress risk factor modification and long-term management. Medications that have been shown to reduce the incidence of future cardiovascular events in patients with acute coronary syndromes include antiplatelet agents, statins, ß-blockers, and angiotensin-converting enzyme inhibitors. Other long-term management strategies include smoking cessation, achievement and maintenance of optimal weight, daily exercise, appropriate diet, and control of hypertension and diabetes.
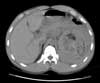
Severe abdominal pain radiating to the back prompted a 72-year-old man to go to the emergency department (ED). The patient had experienced similar pain 2 days earlier and was treated at another hospital for renal colic on the basis of concomitant microscopic hematuria. He had a history of poorly controlled hypertension.
Hypertensive crises encompass a spectrum of clinical situations thathave in common elevated blood pressure (BP) and progressive or impendingtarget organ damage. Each year more than 500,000 Americans (about1% of all persons with hypertension in the United States) have a hypertensivecrisis. In large urban areas, 25% of visits to the medical section of any givenemergency department (ED) are attributable to a hypertensive crisis.
ABSTRACT: The metabolic syndrome, which presents as a cluster of atherogenic traits, confers an increased risk of coronary heart disease (CHD) that may be greater than the sum of the risks associated with the individual components. The principal components of the syndrome are abdominal obesity, elevated triglyceride level, low high-density lipoprotein cholesterol level, elevated blood pressure, and elevated fasting glucose. The presence of 3 of the 5 characteristics establishes the diagnosis. First-line therapy for the metabolic syndrome consists of lifestyle modification measures, such as weight reduction and physical activity; however, pharmacologic treatment may be necessary. Statin therapy decreases the elevated levels of low-density lipoprotein cholesterol and triglycerides characteristic of the metabolic syndrome. Control of nonlipid CHD risk factors, such as hypertension and diabetes, is also critical.
ABSTRACT: Most hypertensive patients require lifestyle modification and multiple-drug therapy to achieve current blood pressure (BP) goals of less than 140/90 mm Hg and less than 130/80 mm Hg for those with diabetes mellitus or renal disease. For patients older than 65 years, the recommended initial antihypertensive is a thiazide diuretic. If a diuretic does not adequately control BP or is contraindicated, base the selection of an antihypertensive medication on comorbid conditions. For example, a ß-blocker may benefit a patient with coronary artery disease, while an angiotensin-converting enzyme inhibitor may help forestall renal disease in a patient with type 2 diabetes mellitus. The adage "start low and go slow" is appropriate to help avoid side effects and ensure compliance; however, most elderly patients eventually require standard dosages of medications to adequately control BP.

For several weeks, a 78-year-old woman had an intensely pruritic, diffuse, raised, slightly scaly, erythematous rash that persisted despite the use of several over-the-counter topical medications (such as hydrocortisone and clotrimazole cream). Since her last visit about 3 months earlier for a blood pressure reading, she had been well except for 2 episodes of night sweats.
A 52-year-old man complains of nausea, fever, and malaise following a 2-day diarrhealillness that developed at the end of a family vacation in New England.Two family members suffered a similar illness, characterized by watery diarrhea.Symptoms developed in all who were affected within 24 hours of eatinghamburgers at a local restaurant.
A 70-year-old man who had just completeda course of trimethoprim-sulfamethoxazolefor a urinary tract infectionpresented with palpable purpuraand cutaneous erosions of acute onseton his legs (A). He also had massivescrotal edema and purpura (B).
A 16-year-old girl was bothered byankle pain and “red spots” on herlower legs. These symptoms clearedin a few days without treatment. Sixweeks later, after returning from anall-day outing at a fair, she noticedthat the spots had reappeared (A)and hemorrhagic lesions had developedon the right ankle (B) and leftheel (C). After removing her shoes,the teenager felt severe pain in bothankles, particularly the right.
A 57-year-old man with a history of venous stasis leg ulcerationwondered about the “white spots” on his leg. Thecondition is atrophie blanche, which manifests as smooth,ivory-white macules and plaques of sclerosis stippled withtelangiectasia that often are surrounded by mild to moderatepigmentation.
Redness, irritation, and diplopia developedover 2 to 3 weeks in a 55-yearoldman’s left eye (A). The injectionworsened and was unresponsive toeye drops. Ptosis, mild proptosis, andelevated intraocular pressure developed.A bruit was auscultated overthe affected eye.
Sudden pain and a pulsatile swellingof the right upper medial thigh concernedan 80-year-old woman (A).Coronary angioplasty had been performedthrough this site 5 weeksearlier.
Four months after a patchy, macular,erythematous spot erupted on thedorsum of a 63-year-old woman’s leftfoot, the area became ulcerated,tender, and painful. The 1.2-cm ulcerwas covered by a hemorrhagic crustsurrounded by a cyanotic reticulardiscoloration of the skin.
A 65-year-old woman, who was confined to a wheelchairbecause of severe rheumatoid arthritis, was concernedabout nodules that had erupted on her fingers and handsduring the previous 3 weeks (A). Her medical historyincluded colon cancer, chronic renal insufficiency, anemia,and hypertension. The nonpruritic nodules were painfulwhen they began to form under the skin; however, oncethey erupted, the pain disappeared.
Advertisement
Advertisement
Trending on Patient Care Online
1
ACOG Releases New Guidance on HIV Screening and Prevention
2
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
3
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
4
FDA Accepts Cefiderocol sNDA for Pediatric Gram-Negative Infections
5