



























































































































































































In the October 2004 issue of TheJournal of Respiratory Diseases,Morrison and Gupta1 reviewed theclinical and laboratory approachesto the diagnosis of communityacquiredpneumonia (CAP) causedby Legionella. They discussed theadvantages and limitations of culture,direct fluorescent antibody(DFA) staining, serology, polymerasechain reaction, and Legionellaurinary antigen assays. As the authorsnoted, DFA staining of respiratorysecretions is an underusedtest that has a high specificity in patientswith untreated Legionnairesdisease.
Pneumonia
Latest News
Advertisement
Advertisement
Abstract: The manifestations of indoor mold-related disease (IMRD) include irritant effects, such as conjunctivitis and rhinitis; nonspecific respiratory complaints, such as cough and wheeze; hypersensitivity pneumonitis; allergic fungal sinusitis; and mycotoxicosis. The diagnosis of IMRD depends on eliciting an accurate history and excluding preexisting pathology that would account for the patient's symptoms. Laboratory tests, imaging studies, and spirometry can play an important role in ruling out other diagnoses, such as allergic or nonallergic rhinitis, asthma, and pneumonia. The diagnosis of IMRD also involves integrating the results of immunologic, physiologic, and imaging studies with the results of indoor air-quality studies. (J Respir Dis. 2005;26(12):520-525)
Templeton and colleagues report encouraging news about the use of polymerase chain reaction (PCR) in the diagnosis of community- acquired pneumonia (CAP). They found that real-time PCR was more sensitive than conventional techniques for detecting major respiratory viruses and atypical bacteria.
Abstract: Acute chest syndrome (ACS) is one of the most common causes of death and hospitalization among patients with a sickle hemoglobinopathy. The clinical presentation is characterized by the appearance of a new infiltrate on a chest radiograph, with 1 or more new symptoms, including fever, cough, chest pain, and dyspnea. Additional findings include leukocytosis, hypoxemia, and auscultatory signs of consolidation. The differential diagnosis includes pneumonia, pulmonary infarction, fat embolism syndrome, pulmonary edema, and bone infarction. Treatment of ACS involves supportive care, empiric antibiotic therapy, and red blood cell transfusion when indicated. The decision of whether to use simple or exchange transfusions depends on the severity of illness and the risk of acute respiratory failure. Currently, hydroxyurea is the only FDA-approved drug designated as a preventive therapy. (J Respir Dis. 2005;26(12):529-534)
Telltale skin lesions of syphilis, gonorrhea, human papillomavirus infection, and Haemophilus ducreyi infection.
The authors describe the development of pneumonitis in a patient who had initially presented with edema of the lower extremities. Biopsy results supported the conclusion that the pneumonitis was caused by silicone injections the patient had received 5 years earlier.
The initial evaluation of a patient with community-acquired pneumonia (CAP) should include a careful search for comorbidities, according to a study by Falguera and associates.
A 45-year-old man presented to the emergency department (ED) with fever and left-sided pleuritic chest pain. He had been in good health until 4 days earlier, when diffuse myalgias, weakness, and frontal headache developed. Two days later, these symptoms were accompanied by onset of fever (temperature, 39.4°C [103°F]) and left-sided pleuritic chest pain. He denied chills, rigors, shortness of breath, hemoptysis, and cough.
An 81-year-old man is seen for follow-up of leukocytosis detected during a recent hospitalization for community-acquired pneumonia. The leukocytosis had not resolved by the time he was discharged.
Progressive cough and dyspnea of 2 months' duration prompted a 23-year-old man to seek medical attention for the fourth time. On previous emergency department visits, he had received antibiotics, which failed to relieve his symptoms.
A 36-year-old woman with a history of HIV disease presented for evaluation of dyspnea of 1 week's duration. She had been taking trimethoprim-sulfa- methoxazole for Pneumocystis carinii pneumonia prophylaxis. Because of a presumed skin reaction to this medication, dapsone was recently substituted.
An erythematous eruption on the eyelids, asymptomatic papules on the extremities, an acneiform rash--can you identify the disorders pictured here?

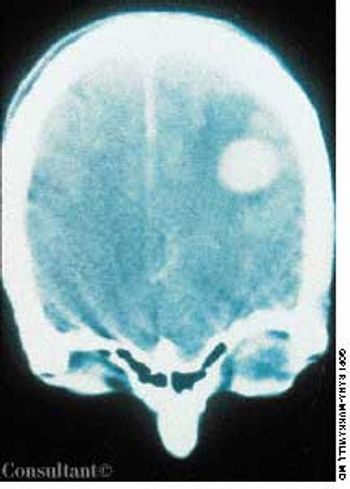
A febrile 65-year-old woman who had suffered a new-onset seizure was brought to the emergency department. The patient-a cigarette smoker-was not coughing and had neither chest pain nor a significant medical history. Her temperature was 39.4°C (103°F). She had nuchal rigidity and Kernig's and Brudzinski's signs of meningeal irritation. Lung auscultation revealed signs of right middle lung consolidation. Her white blood cell count was 1,200/µL. A chest film, seen here, showed a masslike density in the right midlung.

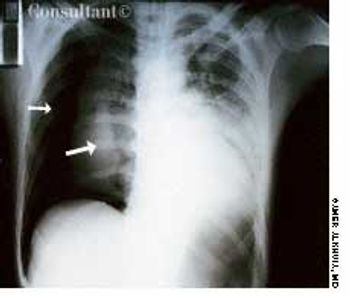
A 35-year-old man, a smoker, had right pleuritic pain, productive cough, and fever for 3 days. His pulse rate was 107 beats per minute; respiratory rate, 14 breaths per minute; blood pressure, 136/80 mm Hg; and temperature, 37.7°C (99.9°F). There were signs of right upper lobe consolidation. Laboratory studies showed hyponatremia. Chest films showed a homogeneous density in the right upper lobe.

A 37-year-old woman presented with progressive dyspnea of 2 weeks' duration, a low-grade fever, and night sweats. She had been a healthy marathon runner until her exercise tolerance recently declined.

A 56-year-old man was admitted to the hospital with right lower lobe pneumonia, which was exacerbated by smoking-induced chronic obstructive pulmonary disease (COPD).
A 32-year-old man who had HIV disease complained of headache, fever, and weakness on his right side. His history included intravenous drug use, Pneumocystis carinii pneumonia, and mucocutaneous candidiasis.
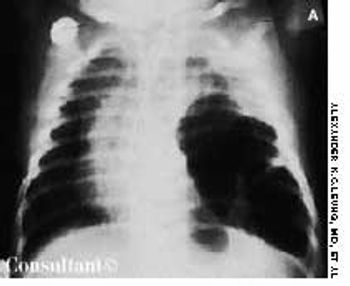
An irritable, lethargic, toxic-looking, and slightly cyanotic 2-month-old boy had a temperature of 40°C (104°F), malaise, and a cough for 2 days. The infant's heart rate was 98 beats per minute, and his respiratory rate was 55 breaths per minute. He had nasal flaring, sternal and subcostal retractions, diminished breath sounds, and scattered rales over the left lung, which was dull to percussion.

A 60-year-old woman with a 3-month history of cough, chest pain, and shortness of breath was brought to the emergency department. The patient denied any history of fever, chills, or rigors; she complained of mild hemoptysis for 1 week and a 9-kg (20-lb) weight loss during the last few months. The patient had smoked cigarettes for 40 years.
A 40-year-old woman with AIDS had been feverish for the past 24 hours and had a nonproductive cough. She had smoked one pack of cigarettes daily for 20 years.

A 25-year-old man, who was an injection drug user, presented with a several-day history of dyspnea and fever. He complained of excessive malaise, fatigue, and weight loss but denied any hemoptysis. The examination of the lung revealed bilateral crackles in both lower zones.

A 43-year-old woman was hospitalized with a 3-day history of fever and back pain. She was malnourished and seropositive for HIV infection. Results of blood and sputum cultures were negative. A community-acquired pneumonia was diagnosed. Chest film findings and the clinical presentation were inconsistent with Pneumocystis carinii pneumonia.

Cough, fever, diarrhea, and weight loss had disturbed a 52-year-old woman for 1 month. AIDS had been diagnosed 5 years earlier, but she had declined medical treatment. The patient's vital signs were stable when she was admitted to the hospital. Physical examination results were unremarkable except for thrush and mild, diffuse abdominal tenderness.

Purplish skin lesions appeared on the back and trunk of a 34-year-old homosexual man with HIV-1 disease. The spots had been growing larger over the past several weeks.
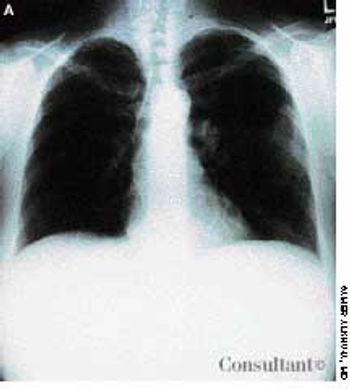
While watching TV, a 32-year-old man experienced acute right-sided pleuritic pain and was taken to the emergency department. He was seropositive for HIV but had never had Pneumocystis carinii pneumonia (PCP) and was not taking aerosolized pentamidine. Physical examination revealed hyperresonance with significantly decreased breath sounds over the right hemithorax.
Advertisement
Advertisement
Trending on Patient Care Online
1
Artificial Intelligence ECG Model Identifies Patients at Higher Risk for Sudden Cardiac Death
2
Cognitive Rehabilitation Linked to Functional Gains in Long COVID Trial
3
Telehealth Mindfulness Program Linked to Sustained Low Back Pain Improvements
4
FDA Authorizes Modified Risk Claim for ZYN Nicotine Pouches
5