



























































































































































































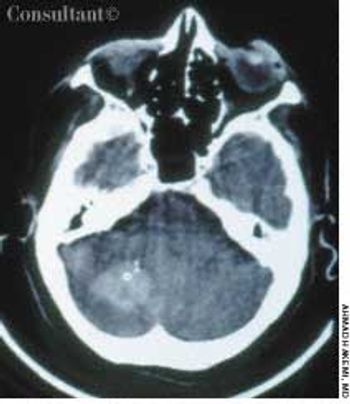
A Young Boy With High Fever and LethargyA 5-year-old boy is brought to the emergency department(ED) by his parents. They report that, for thepast week, the child has had a high fever (temperatureup to 40oC [104oF]), generalized weakness, lethargy, andlack of appetite. The boy’s eyes are bloodshot and he hasrefused food and drink. The child has no history ofcough, shortness of breath, hematemesis, melena, headaches,vision problems, or seizures. He has not been incontact with sick persons, has not traveled abroad, doesnot have a pet, and is not taking any medications. His immunizations are up-to-date.
Atrial Fibrillation
Latest News
Advertisement
Advertisement
ABSTRACT: Topical agents can provide temporary relief from osteoarthritis symptoms with little or no risk. Acetaminophen is first-line oral therapy. Be alert for risk factors for NSAID-induced GI toxicity, such as concurrent use of prescription and OTC agents. Tramadol, narcotic analgesics, muscle relaxants, and antidepressants are options when NSAIDs are ineffective or contraindicated. Intra-articular injections of corticosteroids or hyaluronan are appropriate for patients who have a single joint exacerbation. Total knee and total hip arthroplasty are considered the most effective surgical interventions.
Cardiac stress imaging has become increasingly sophisticated; nevertheless, standard exercise electrocardiography can provide valuable clinical information, such as time to onset of angina or ST-segment depression, maximal heart rate and blood pressure response, and total exercise duration. Pharmacologic stress agents may be substituted for patients who cannot exercise on a treadmill; however, these agents must be used in conjunction with echocardiography or nuclear scintigraphy to obtain adequate diagnostic information.
How critical-and cost-effective-is in-officepulmonary function equipment for the primarycare practitioner?
A 41-year-old woman has had a 2-week bout of nausea, vomiting, and diarrhea.Her history includes chronic hepatitis C and alcohol abuse. She also has orthostatichypotension. A baseline ECG is obtained.
ABSTRACT: The main therapeutic goals for patients who have an acute coronary syndrome are to reestablish normal epicardial flow and to increase distal myocardial perfusion. Fibrinolytic treatment with tissue plasminogen activator within 70 minutes of the onset of symptoms dramatically reduces the mortality rate from myocardial infarction. Other fibrinolytic agents include reteplase, which is given as a double bolus, and tenecteplase, which is given as a single bolus. In most hospitals, fibrinolytic therapy is more readily available than percutaneous transluminal coronary angioplasty (PTCA); however, PTCA may be the preferred approach if it is available within an hour and a half. Antiplatelet drugs, such as glycoprotein IIb/IIIa receptor antagonists, are used to improve distal myocardial perfusion. If follow-up coronary angiography is not available to assess whether epicardial blood flow and distal myocardial perfusion have been restored, a 12-lead ECG can provide valuable information. The resolution of ST-segment abnormalities is a marker for improved perfusion.
ABSTRACT: Patients can greatly reduce the risk of traveler's diarrhea by drinking only bottled water and eating only hot foods prepared in sanitary conditions or peelable fruits and vegetables. Antibiotic prophylaxis for traveler's diarrhea is no longer routinely recommended; reserve it for patients who may have to consume food and beverages of questionable safety, those with reduced immunity, and those likely to experience serious consequences of illness. Adequate hydration is the first step in treating traveler's diarrhea. Drug therapy-loperamide or fluoroquinolones in adults and bismuth subsalicylate or azithromycin in children-can ameliorate symptoms and speed recovery. Recommend that patients who are prone to motion sickness take an antiemetic/antivertigo agent before symptoms begin. Acetazolamide can be used both to prevent and to treat altitude sickness. Contraindications to air travel include a resting oxygen saturation of less than 90%, pregnancy of more than 36 weeks' duration, pneumothorax, recent myocardial infarction or chest or abdominal surgery, active infectious diseases, and poorly controlled seizures or sickle cell anemia.
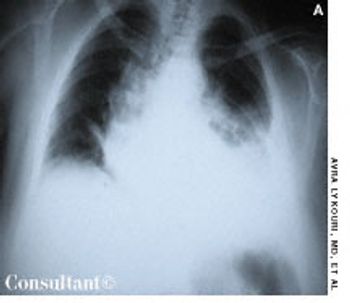
A 78-year-old man presented to theemergency department with a 3-weekhistory of progressive shortness of breathand cough with blood-streaked, yellowishsputum. The patient had dyspnea onexertion limited to 2 blocks, 2-pilloworthopnea, paroxysmal nocturnal dyspnea,and nocturia. Neither fever norchills were present. He had lost 7.2 kg(16 lb) during the last year.
A 77-year-old man is brought to the emergency department after severaldays of illness that began with fever, nausea, emesis, and headache. Muscleweakness and associated myalgia developed; the weakness became so severethat the patient needed help to get out of bed and walk to the bathroom.The day before he came to the hospital, he slept much of the time and wasdifficult to arouse.

A 48-year-old woman was admitted to the hospital with deep venous thrombosis of the right leg. She had a history of non-Hodgkin lymphoma, which was in remission. The patient had been a heavy smoker for many years.
A 69-year-old retired accountant presents with a 2-month history of daily headaches. The pain is moderate, constant,global, pressure-like, and occasionally pulsating; it is sometimes exacerbated when the patient lies down. He denies nauseaor vomiting, ocular symptoms, weakness, or sensitivity to light. His wife reports that years ago he experienced throbbingheadaches regularly.
ABSTRACT: A key objective in the follow-up of women with a history of breast cancer is the detection of local and distant disease at a curable stage. Regular clinical examination and yearly mammography are the standard of care. No consistent evidence supports annual chest radiography, bone scans, or tests of serum tumor markers. Order laboratory or diagnostic tests only if indicated by clinical findings. Advise women to report new symptoms promptly rather than waiting for the next scheduled examination. Some evidence supports the use of venlafaxine for tamoxifen-associated hot flashes. Despite the increased incidence of endometrial carcinoma in women taking tamoxifen, routine endometrial biopsies are not recommended. Most experts advise that women with a history of breast cancer who wish to have a child wait 2 to 3 years before becoming pregnant.
ABSTRACT: Age-related anatomic and physiologic alterations in the thyroid gland have a variety of clinically important effects. Hypothyroidism, which is common in older persons, raises cholesterol and triglyceride levels; hyperthyroidism may be masked by the severity of the cardiac problems it causes. In younger persons, depression may accompany hypothyroidism but not hyperthyroidism; however, in the elderly, it may be a feature of either condition. Papillary carcinoma-the most common type of thyroid cancer-is more aggressive in older persons. All these factors necessitate a cautious and deliberate approach to the management of thyroid disorders in elderly patients.
During a routine office visit, a 64-year-old woman who has had type 2 diabetesfor more than 10 years complains of increased pedal edema. The edema is minimalon awakening and worsens throughout the day.
More than1.8 millioncardiaccatheterizationsandat least 600,000 percutaneoustransluminal coronaryangioplasty (PTCA)procedures are performedin the United States annually.1 The use of these diagnosticand interventionalmodalities continues togrow even as financial constraintsincrease. Yet formany patients with coronaryartery disease (CAD),medical therapy may be anappropriate option.
ABSTRACT: For patients who present with ventricular fibrillation (VF) or pulseless ventricular tachycardia that is refractory to repeated countershocks, the drug of choice is amiodarone; the recommended dose for those who are receiving cardiopulmonary resuscitation is 300 mg given as an IV bolus. Vasopressin, 40 U IV, is an acceptable alternative to epinephrine in adults with VF that is resistant to electrical defibrillation. Standard heparin or low molecular weight heparin is indicated in patients who require reperfusion therapy and in those who have unstable angina or non-Q wave myocardial infarction (MI). The initial therapy for patients with acute myocardial ischemia usually includes morphine, oxygen, nitroglycerin, and aspirin, plus a ß-adrenergic blocking agent. Glycoprotein IIb/IIIa receptor inhibitors are currently recommended for patients who have non-Q wave MI or high-risk unstable angina.

For 2 days, a 68-year-old woman had watery, yellowish diarrhea with mucus and left lower quadrant pain. Her medical history included hypertension, diabetes mellitus, and congestive heart failure (CHF); she had left the hospital 5 days earlier following treatment of an exacerbation of CHF with intravenous furosemide and sodium and fluid restriction. The patient was taking furosemide, lisinopril, and glipizide; she denied any recent antibiotic therapy.

A 64-year-old woman with a history of diabetes, hypertension, and lymphoma was admitted to the hospital with a dull headache, conjunctival congestion, and slight dyspnea. Her pulse rate was 96 beats per minute; blood pressure, 146/68 mm Hg; and respiration rate, 22 breaths per minute. She also had increased jugular venous distention; cardiovascular and chest examination findings were normal. Edema of both arms and dilated blood vessels on the anterior chest wall were noted.
This simple technique can quickly reduce leg edema. Instruct the patient to place a chair on abed as shown, lay a pillow on the back of the chair, then lie down with legs elevated on the pillowcoveredchair back. (Do not use in patients with congestive heart failure; volume overload andpulmonary edema may result.)
A 65-year-old woman with a long history of hypertension treated with metoprolol and felodipine complained of dizziness, headache, nausea, and vomiting of acute onset. Her blood pressure was 220/110 mm Hg. She was drowsy and unable to stand or walk.
Heart failure(HF), the mostcommon Medicarediagnosisrelatedgroup,has a significant and growingimpact on health careresources. The incidenceof HF has tripled during thelast decade. Almost 5 millionAmericans have HF, and anestimated 500,000 new casesare diagnosed yearly. Thelifetime risk of HF is about20%.1 Drug therapy has improvedconsiderably in recentyears, but the magnitudeand severity of theproblem has created a needfor newer therapies--particularlysince HF is associatedwith an increased risk ofsudden death and a diminishedquality of life.2
A 58-year-old man recently underwent coronary artery bypass graft (CABG)surgery after emergent cardiac catheterization for a myocardial infarction revealeddiffuse 3-vessel disease.
A 65-year-old woman experienced dyspnea, dizziness, and left pleuritic pain several hours after falling down a flight of stairs. Shallow breathing and increased tenderness of the left thoracic wall were evident with palpation. Decreased breath sounds on the left and dullness on percussion were also noted.
Long-term oxygen therapy (LTOT) improves both the length and qualityof life of hypoxemic patients with COPD. It is the only therapy thatclearly increases survival for selected patients with advanced stable COPD.
For 2 days, a 79-year-old man with a history of congestive heart failure experienced abdominal pain, diarrhea, and dark red rectal bleeding. The pain was localized to the left lower quadrant.
Advertisement
Advertisement
Trending on Patient Care Online
1
Artificial Intelligence ECG Model Identifies Patients at Higher Risk for Sudden Cardiac Death
2
Cognitive Rehabilitation Linked to Functional Gains in Long COVID Trial
3
Telehealth Mindfulness Program Linked to Sustained Low Back Pain Improvements
4
FDA Authorizes Modified Risk Claim for ZYN Nicotine Pouches
5