




























































































































































































ABSTRACT: Most hypertensive patients require lifestyle modification and multiple-drug therapy to achieve current blood pressure (BP) goals of less than 140/90 mm Hg and less than 130/80 mm Hg for those with diabetes mellitus or renal disease. For patients older than 65 years, the recommended initial antihypertensive is a thiazide diuretic. If a diuretic does not adequately control BP or is contraindicated, base the selection of an antihypertensive medication on comorbid conditions. For example, a ß-blocker may benefit a patient with coronary artery disease, while an angiotensin-converting enzyme inhibitor may help forestall renal disease in a patient with type 2 diabetes mellitus. The adage "start low and go slow" is appropriate to help avoid side effects and ensure compliance; however, most elderly patients eventually require standard dosages of medications to adequately control BP.
Atrial Fibrillation
Latest News
ABSTRACT: Because physical findings are an unreliable indicator of deep venous thrombosis (DVT), the diagnosis is based on the presence of clinical risk factors and the results of noninvasive tests, such as duplex ultrasonography and impedance plethysmography. Contrast venography is considered the gold standard for the diagnosis of DVT. Uncomplicated DVT is managed with low molecular weight heparin followed by warfarin. When DVT is complicated (eg, by pregnancy or by evidence of pulmonary embolism), the patient is treated with intravenous heparin; the dosage is adjusted to achieve an activated partial thromboplastin time 3 times control. Chronic venous insufficiency is the most common cause of leg ulcers. Treatment goals include reduction of edema, relief of pain, ulcer healing, and prevention of recurrence. Leg elevation and multilayer elastic compression dressings are the mainstays of therapy. Compression dressings are continued until ulcers heal; graded compression stockings are worn to prevent recurrence. Pentoxifylline, 400 mg 3 times a day, is an effective adjunct to compression bandaging. Large or slow-healing ulcers may require skin grafts.
ABSTRACT: Thrombolysis with intravenous tissue plasminogen activator (tPA), administered within 3 hours of symptom onset, is the only FDA-approved treatment for acute ischemic stroke. Recently, intra-arterial prourokinase was found to improve recanalization and clinical outcome when administered to select patients up to 6 hours after symptom onset. Combination intravenous/intra-arterial thrombolysis can compensate for the delays that are often associated with intra-arterial therapy (products of the paucity of qualified centers and the time required for angiography). Increased risk of hemorrhagic transformation is associated with all routes of thrombolytic administration. However, greater awareness of specific risk factors for hemorrhagic transformation-especially newer CT and MRI criteria-may enable physicians to select patients with an optimal chance of benefiting from thrombolytic therapy, and may also extend the therapeutic window. Despite the higher rate of hemorrhagic transformation, thrombolytic therapy has demonstrated a significant benefit in the treatment of patients with acute stroke.
Every minute, an American woman dies of cardiovascular disease (CVD), the leading cause of death among women in the United States. Each year, more than half a million women die of cardiovascular causes, including 250,000 of coronary heart disease.Despite the prominent reduction in cardiovascular mortality in the United States among men, mortality has not decreased recently among women. Since 1984, CVD has killed more American women than men every year.1,2
ABSTRACT: The auscultatory features of heart murmurs-intensity, frequency, quality, configuration, timing, duration, and radiation-can help identify a variety of cardiac disorders. Systolic ejection murmurs have a crescendo-decrescendo configuration. These include innocent murmurs and those associated with aortic stenosis and hypertrophic cardiomyopathy. Systolic murmurs associated with retrograde flow from a high-pressure chamber to a low-pressure chamber usually have a holosystolic configuration. Examples of holosystolic murmurs include mitral regurgitation, tricuspid regurgitation, and the murmur associated with a ventricular septal defect. Diastolic murmurs include regurgitant murmurs, such as the decrescendo murmur of aortic regurgitation, and filling murmurs, such as the presystolic rumble of mitral stenosis, which is preceded by an opening snap. The murmur associated with patent ductus arteriosus is continuous.
Numerous factors put elderly patients at risk for adverse drug events. On average, they take at least 6 medications a day, which increases the likelihood of drug-drug interactions. In addition, many drugs that are safe and effective in younger patients are inappropriate for older persons because of age-related changes and comorbid conditions that affect absorption, distribution, metabolism, and elimination. First-pass metabolism decreases with age, which may increase systemic absorption of some oral nitrates, ß-blockers, estrogens, and calcium channel blockers. The age-related rise in body fat increases the volume of distribution of lipid-soluble compounds, such as diazepam, and prolongs clearance. About two thirds of elderly persons have impaired kidney function; in these patients, the dosage of renally excreted drugs-such as digoxin-needs to be reduced. Other strategies for avoiding adverse drug events are detailed here.
To distinguish between hypertensive emergencies and urgencies and nonurgent acute blood pressure elevation, evaluate the patient for evidence of target organ damage. Perform a neurologic examination that includes an assessment of mental status; any changes suggest hypertensive encephalopathy. Funduscopy can detect papilledema, hemorrhages, and exudates; an ECG can reveal evidence of cardiac ischemia. Order urinalysis and measure serum creatinine level to evaluate for kidney disease. The possible causes of a hypertensive emergency include essential hypertension; renal parenchymal or renovascular disease; use of various illegal, prescription, or OTC drugs; CNS disorders; preeclampsia or eclampsia; and endocrine disorders. A hypertensive emergency requires immediate blood pressure reduction (although not necessarily to the reference range) with parenteral antibiotics. An urgency is treated with combination oral antihypertensive therapy.
ABSTRACT: The basic screening studies for rheumatic diseases are a complete blood cell count, a determination of the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) level, a rheumatoid factor assay, an antinuclear antibody (ANA) test, a measurement of serum uric acid level, and a urinalysis. Test results must be interpreted within a clinical context; for example, a positive ANA assay suggests the possibility of a rheumatic disorder, but it is not specific for any diagnosis. Tests that reveal the nature and extent of target-organ involvement, such as renal function studies in patients with systemic lupus erythematosus, can help guide the selection of therapy. Laboratory results also reflect disease activity; the ESR and CRP level are useful gauges of the activity of most inflammatory rheumatic disorders. Finally, laboratory monitoring can help you minimize the significant toxicity associated with many of the drugs used to manage rheumatic diseases.
Numerous factors contribute to the medication errors that kill up to 98,000 patients each year. Unnecessarily high dosages can result in increased side effects with only a small therapeutic benefit, especially in elderly patients. Lack of patient information-such as a history of allergies or adverse drug reactions-is another cause of error and injury. Communication failures include the use of ambiguous abbreviations, misinterpretation of verbal orders, and lack of timely response to a patient's medication-related symptoms. Dosing errors are common in children because of variability in dosage expressions in drug references. Remedies for prescribing errors are described in detail here.
A methodical approach to diagnosis usually reveals the cause of fever. In patients with simple fever, a careful history taking and physical examination combined with basic laboratory and imaging studies (complete blood cell count with differential, urinalysis, and possibly a chest film and blood cultures) usually yield the diagnosis. In patients with prolonged fever whose cause remains undiagnosed after extensive examination (fever of unknown origin), repeat the history taking and physical examination; also order routine laboratory studies, an HIV test, a tuberculin skin test, 3 sets of blood cultures, and chest films. In addition, abdominal CT scanning is often useful. Further testing at this point may include fluorodeoxyglucose positron emission tomography, technetium-tagged white blood cell scanning, transesophageal echocardiography, liver biopsy, bone marrow examination, and/or temporal artery biopsy. Exploratory laparotomy is rarely indicated.
Q:Which combinations of antihypertensivemedications are most effective-and which arebest avoided?
A 75-year-old obese woman with subacute-onset dyspnea and lower right posterior chest pain was brought to the emergency department. She had a history of diastolic heart failure, arthritis, and suspected obstructive sleep apnea. The patient was dyspneic at rest.
ABSTRACT: Diuretics remain a mainstay of heart failure therapy. Angiotensin-converting enzyme (ACE) inhibitors and ß-blockers inhibit activation of neurohormonal systems; these agents are recommended for most patients with symptomatic systolic heart failure. Angiotensin II receptor blockers (ARBs) are alternatives for patients who are unable to tolerate ACE inhibitors. Recent trials suggest that ARBs are also useful when added to the regimen of patients with a low ejection fraction. Although digoxin can provide long-term inotropic support in men, it significantly increases the risk of mortality in women; because of the risk of toxicity, use digoxin with caution in older persons and patients with renal dysfunction. Consider an aldosterone antagonist in patients who remain symptomatic at rest despite the use of a diuretic, digoxin, an ACE inhibitor or an ARB, and a ß-blocker. Lifestyle modifications such as dietary restriction and exercise are helpful in all patients.
Your patient with type 2 diabetes wants to take a step exercise class. What recommendations will you offer? Another patient has diabetic retinopathy; which exercises are safest for her?
ABSTRACT: In high-risk patients with vascular disease, blockade of the renin- angiotensin system (RAS) can help prevent cardiac remodeling that ultimately results in left ventricular hypertrophy (LVH) and heart failure. Optimal treatment of these patients, who often have diabetes or renal disease, usually involves a combination of agents-1 of which should be a thiazide diuretic-to reduce blood pressure, control the comorbid condition, and prevent end-stage organ damage. The manner in which the RAS is interrupted may be important. For example, although a thiazide diuretic and an angiotensin-converting enzyme (ACE) inhibitor are recommended for hypertensive patients with LVH, an angiotensin II receptor blocker (ARB) in combination with a diuretic was recently found to reduce cardiovascular morbidity and mortality in these patients to a greater degree than a ß-blocker/diuretic. Both ACE inhibitors and ARBs delay the progression of diabetic nephropathy and reduce albuminuria. ARBs were recently shown to reduce progression from microalbuminuria to macroalbuminuria. In patients with systolic heart failure who cannot tolerate ACE inhibitors, an ARB can be used with a ß-blocker.
ABSTRACT: Many patients with presumed mild intermittent asthma have unrecognized persistent symptoms; these can be elicited with specific questioning about coughing, wheezing, shortness of breath, chest tightness, nighttime awakenings, and exercise intolerance. Asthma severity may vary with the season. For asthmatic patients with predictable seasonal allergies, prescribe inhaled corticosteroids for a few weeks or months beginning 2 to 3 weeks before usual symptom onset. Successful long-term management requires identification and control of asthma triggers, such as cigarette smoke, house dust mites, cockroaches, molds, and animal dander. Removing triggers or minimizing the patient's exposure to them may allow improved asthma control with lower dosages of corticosteroids.
Persons with a systolic blood pressure (BP) of 120 to 139 mm Hg or a diastolic BP of 80 to 89 mm Hg are now considered, according to the latest Joint National Committee (JNC) report on hypertension.
ABSTRACT: To identify the cause of hyponatremia, determine the patient's volume status and measure urinary sodium and osmolality; also ask about diuretic use. Hypovolemic hyponatremia is associated with vomiting, diarrhea, laxative abuse, renal disease, nasogastric suction, salt-wasting nephropathy, Addison disease, solute diuresis, and diuretic use. Euvolemic hyponatremia with a normal urinary sodium level can result from glucocorticoid deficiency, hypothyroidism, certain drugs, and the syndrome of inappropriate antidiuretic hormone secretion. Euvolemic hyponatremia with low urinary osmolality can be caused by psychogenic polydipsia, "tea and toast" syndrome, or beer potomania. Hypervolemic hyponatremia is associated with congestive heart failure, nephrotic syndrome, and cirrhosis. To reduce the risk of serious neurologic sequelae, avoid both undertreatment and overtreatment of hyponatremia. In chronic hyponatremia, total correction should not exceed 8 to 12 mEq/L/24 h (a maximum correction rate of 0.5 mEq/L/h). In acute hyponatremia, rates of correction up to approximately 1 mEq/L/h are acceptable. Avoid overcorrection of serum sodium concentration (ie, to a level higher than 140 to 145 mEq/L).
The cardioprotective benefits of marine-derived omega-3 fatty acids in persons with cardiovascular disease (CVD) as well as in healthy persons have been documented in recent randomized, controlled clinical trials.
ABSTRACT: Effective smoking cessation strategies typically encompass the use of some pharmacotherapy with counseling by physicians. Give the Fagerstrom test to patients who want to quit smoking to determine their degree of nicotine dependence. For low-nicotine-dependent smokers, the use of 1 smoking cessation product for a short period has proved successful; for high-dependence smokers, a combination of products, such as nicotine gum and a nicotine patch, can be used. Other available smoking cessation products are the nicotine nasal spray, the nicotine inhaler, and sustained-release bupropion. Increasing the dose or duration of nicotine gum and patch has improved abstinence rates among high- dependence smokers. Quit rates have also been shown to increase with the dose of bupropion.
ABSTRACT: In addition to advanced age, factors such as comorbid illness and debility determine the risk of community- acquired pneumonia (CAP). Many elderly persons do not have the classic symptoms of CAP; instead, they may present with confusion, lethargy, tachypnea, anorexia, or abdominal pain. Even with thorough investigation, an infectious pathogen can be identified in only about half of patients. In addition to the causative organisms for pneumonia in younger adults, elderly persons are at risk for infection with organisms such as Haemophilus influenzae, Staphylococcus aureus, enteric gram-negative bacteria, and anaerobes, and for polymicrobial infection. Prompt empiric treatment is essential. Recommended initial therapy choices include a ß-lactam agent with a macrolide, or an antipneumococcal fluoroquinolone.
ABSTRACT: Recent studies, although suggestive, do not yet support the routine use of angiotensin II receptor blockers in combination with angiotensin-converting enzyme (ACE) inhibitors in patients with congestive heart failure (CHF). For CHF patients in normal sinus rhythm, consider digoxin when a regimen of diuretics, ACE inhibitors, and β-blockers at optimal dosages does not relieve symptoms completely. Anticoagulation may be warranted in CHF patients with atrial fibrillation, previous embolic events, severely reduced systolic performance, or potential chamber clots. β-Blockers are indicated for patients with mild to severe CHF, unless there is a specific contraindication, and therapy should be initiated once euvolemia has been achieved. Avoid NSAIDs and cyclooxygenase-2 inhibitors in patients with CHF because the prostaglandin-blocking properties of these agents may promote fluid retention.
For several days, a 60-year-old woman has had fever, myalgias,fatigue, poor appetite, and diminished oral intake. Shedenies cough, sputum production, and urinary symptoms.
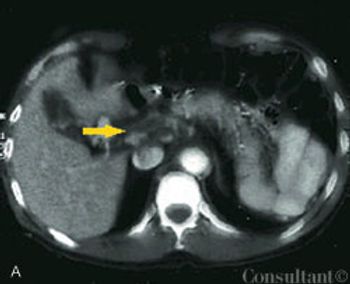
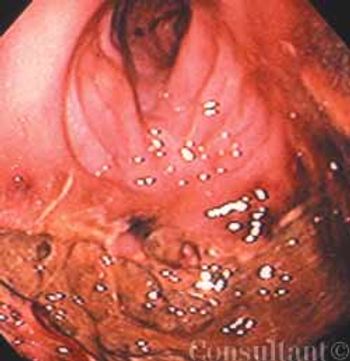
A 60-year-old man presented to the emergency department (ED) with fever of 1 day’s duration and midabdominal pain. The cramping pain had begun 3 days earlier in a bandlike distribution around the upper abdomen. Ingestion of food exacerbated the discomfort. The patient had a history of intermittent constipation; he denied alcohol or illicit drug use, nausea, vomiting, and weight loss. He did not use any herbal or over-the-counter medications.
Sir William Osler once called pneumococcalpneumonia “the captain of themen of death.”1 Pneumonia is the sixthleading cause of death in the UnitedStates and the fourth leading causeamong Americans 80 years of age andolder.2