





























































































































































Conjunctivitis, iritis, ocular vaccinia, herpes zoster ophthalmicus-a few of the conditions for which patients seek treatment every day.
Conjunctivitis, iritis, ocular vaccinia, herpes zoster ophthalmicus-a few of the conditions for which patients seek treatment every day.
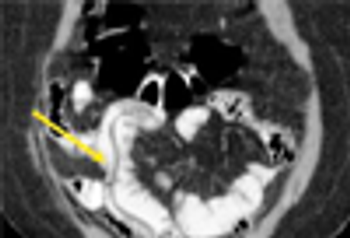
Emphysematous cholecystitis is a rare condition that is the result of infection with C perfringens and other gas-producing organisms including Escherichia coli, Bacteroides fragilis, and Klebsiella species.
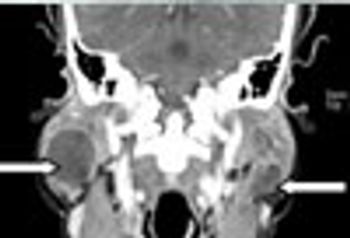
Lymphoepithelial cysts of the parotid gland may be diagnostic of HIV infection; they are typically bilateral, benign, and associated with lymphadenopathy.
Patients with ulcerative colitis and Crohn’s disease typically don’t receive preventive services at the same rate as general medical patients. Vaccination is a key area of confusion.

(AUDIO) There are disparities in the sensitivities and specificities of glucose and lactose hydrogen breath tests used to diagnose small intestine bacterial overgrowth and to distinguish patients with irritable bowel syndrome from healthy individuals. Just how useful are these tests? Insights from an expert here.
If you are worried about whether you may have injected a patient with a tainted vial of methylprednisolone from New England Compounding Center’s (NECC) Framingham, Massachussets facility, you can now obtain detailed information from the FDA that may assuage your concerns.
Here: an update on the challenges of detection, diagnosis, and management of celiac disease and non–celiac disease and the importance of gluten sensitivity.
Despite warnings and concerns, the evidence points to this bottom line: PPIs are relatively safe over the long term.

Always check the toenails for fungal infection after diagnosing tinea pedis, corporis, or cruris. The toenails may act as the source of infection and a reservoir, which may lead to reinfection after the cutaneous dermatophytosis is cleared.
Age-based screening recommendations for chronic hepatitis C virus infection targeted to Americans born between 1945 and 1965 were announced by the CDC.
It is high season for this potentially deadly viral infection, cases of which have been reported in every state. Will you be prepared? Guidance here from an expert.
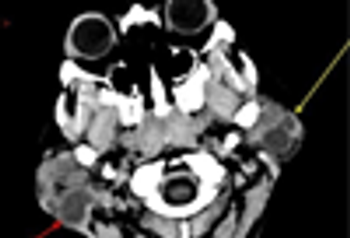
A large minority of persons with HIV infection have head and neck symptoms; parotid swellings have been noted in approximately 5% to 10% of patients with HIV-1 infection.
Although genetics risk explains the familial clustering of MS, it cannot fully explain the geographic distribution of MS and the changes in risk that occur with migration. Infections have been suggested as a possible explanation. The most convincing candidate for involvement in MS is the Epstein-Barr virus.

Syphilis is often called the "great imitator." The slides that follow show syphilis in various guises-and various disorders that can mimic the cutaneous manifestations of the sexually transmitted infection.
Intestinal helminthes represent one of the most prevalent types of human parasitic disease and remain a major health problem in developing countries.

These whitish colored lesions were the result of lichen planus. Hepatitis C virus infection should be sought, since this viral infection is often associated with recent-onset lichen planus in younger persons.

The patient knew that he had psoriasis, but failed to connect onychodystrophy to his underlying skin disease.

Pitted keratolysis is caused by pedal hyperhidrosis and subsequent overgrowth of bacteria that produce proteinases that dissolve keratin and lead to pit formation.
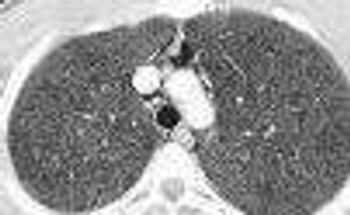
Spontaneous pneumomediastinum with subcutaneous emphysema is rare. Alveolar rupture allows air to enter the pulmonary interstitium and penetrate the mediastinum.
For many patients with diabetic peripheral neuropathy, severe pain can be controlled to a degree sufficient to improve their quality of life. Here: effective management strategies, including topical agents, oral medications, and nonpharmacological therapies (eg, acupuncture and transcutaneous nerve stimulation).
Common MS exacerbation triggers: infection, vaccination, stress, smoking, vitamin deficiency, or environmental changes.

This was presumed to be an ectoparasite bite when the patient reported that she had a new pet kitten. A myriad of diagnostic possibilities exist, including the start of a drug eruption or viral infection, early allergic contact dermatitis, or first manifestation of an autoimmune bullous disease.

Epidermoid cysts may be treated with intralesional injections of phosphatidylcholine to avoid potential recurrence, eliminate scarring, and reduce cost.

Autosomal dominant polycystic kidney disease (ADPKD) is common. Presenting symtpoms include hypertension, hematuria, proteinuria, and renal insufficiency.
For most patients who have had low back pain for less than 6 weeks, there is little need for imaging studies.