




































































































































































One of the keys to successfully managing acute pulmonary embolism (PE) is to quickly and reliably identify which patients require anticoagulant therapy. A diagnostic algorithm that combines clinical probability, D-dimer results, and CT findings appears to be quite effective in achieving this, according to a multicenter study conducted in the Netherlands.
Cerebrovascular Diseases
Latest News
Advertisement
Advertisement
Excess weight increases the risk of having a heart attack, stroke, high blood pressure, arthritis, diabetes, depression, fatigue, and certain types of cancer. Losing weight and keeping it off are very difficult for most persons who are overweight. Here are some suggestions to help you lose pounds and keep your weight down.
n the first 7 days after a transient ischemic attack (TIA), the risk of a stroke is 10%.1 If half the patients who presented with TIAs were admitted and received an immediate workup within that 7-day window, only 5% of them would have a stroke.1 Thus, many patients would undergo unnecessary tests. Some would have complications, and the costs would be prohibitive. What is needed is a way to identify patients who are at high risk for a stroke in the immediate future--and who require emergent assessment.
To help patients who have had a cerebrovascular accident regain fine motor skills and hand-eye coordination, have them cut out manufacturers' coupons with blunt-edged scissors
Heparin-induced thrombocytopenia (HIT) is a potentially life-threatening complication that occurs in about 1% to 5% of patients who receive heparin.1 Patients with HIT are at risk for the development of new thrombosis, including pulmonary embolism (PE). The mortality rate among patients with HIT and thrombosis is about 20% to 30%.2-5
Abstract: Many patients with sarcoidosis are asymptomatic at presentation and have bilateral hilar adenopathy on a chest radiograph obtained for other reasons. Symptomatic patients usually present with chronic cough, dyspnea, or noncardiac chest pain. Extrapulmonary organ involvement is not uncommon. Lung biopsy shows well-formed noncaseating granulomas in a bronchovascular distribution. Interstitial lung disease also may result from collagen vascular disease, such as systemic lupus erythematosus and Sjögren syndrome. In patients with acute hypersensitivity pneumonitis, cough, dyspnea, and flu-like symptoms occur within 12 hours of exposure to the inciting antigen, such as pigeon stool or moldy hay. Some patients have a subacute or chronic course, probably as a result of continued exposure to the offending antigen. In acute hypersensitivity pneumonitis, the chest radiograph may show diffuse small nodules, whereas in chronic disease, reticular lines or fibrosis may be seen. (J Respir Dis. 2005;26(10):443-448)

This is a multisystem disorder characterized by oral and genital aphthae. Other symptoms include a myriad of cutaneous findings; variable systemic features include uveitis, synovitis, meningoencephalitis, and large- and smaller-vessel vascular disease.

A 72-year-old woman had complained of shortness of breath for the past week. A CT scan showed a large filling defect in the left main pulmonary artery (Figure A, thin arrows) that extended into both the upper and lower branches. Another filling defect (not shown here) was seen along the posterior wall of the right main pulmonary artery, extending into the lower branch. These defects are compatible with pulmonary emboli.
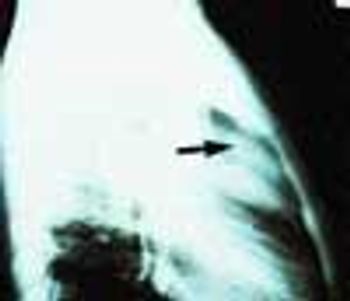
A 72-year-old woman who had fallen and injured the left side of her chest came to the emergency department complaining of pain in that area. She was physically stable and not short of breath. A soft systolic murmur was heard over the left precordium; the lungs were clear. A posteroanterior chest film showed no rib fracture but it did show an enlarged heart and a large, calcified ventricular aneurysm.

A 52-year-old woman who was undergoing chemotherapy for lymphoma was admitted to the hospital with fever of a few days' duration. The patient had smoked cigarettes for many years; she had no history of deep venous thrombosis.

For 2 months, a 31-year-old woman had had dyspnea and dull, continuous retrosternal pain. She was admitted to the hospital, and a helical CT scan of the thorax identified a saddle pulmonary embolism. An ultrasonogram revealed deep venous thrombosis (DVT) in the left leg. Intravenous heparin was given; the patient was discharged, and warfarin was prescribed.

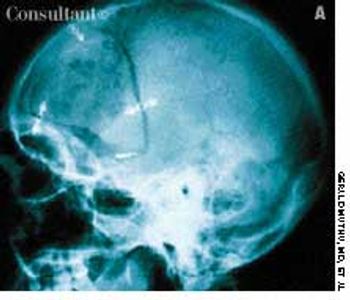
Increasingly frequent headaches and blurred vision had affected a 74-year-old woman for several months. Double vision, which initially occurred only when the patient looked to the right, had started to affect vision when she looked straight ahead. Her eye movements when looking to the left were normal; the right eye, however, did not go beyond midline when looking to the right. Upward and downward gaze were not affected.
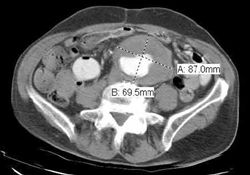
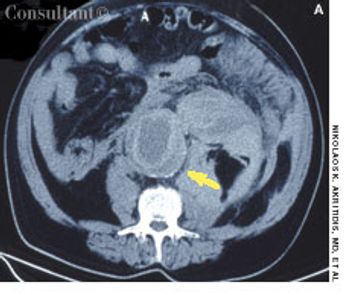
A 53-year-old woman had complained of pain in the lower right quadrant of her abdomen for 1 year. She claimed that the pain intensified when she bent forward in a particular position but believed it was unrelated to food, bowel movements, or urination. There was no weight loss, vomiting, or melena. There was no family history of colon cancer or inflammatory bowel disease.
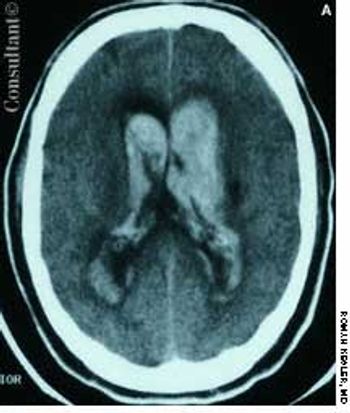
A 57-year-old man complained of a severe headache of sudden onset while he was lifting heavy boxes. Within minutes, he collapsed and became unconscious. On arrival at the emergency department, the patient was deeply comatose. His pupils were 7 mm, fixed, and unreactive to light; brainstem reflexes were absent, and he was unresponsive to noxious stimulation. His blood pressure was 210/120 mm Hg; he had no known history of hypertension.

A 75-year-old woman with a bioprosthetic aortic valve, who had undergone surgical repair of an aortic root aneurysm 9 months earlier was hospitalized with fever, headache, and altered mental status of 1-day's duration.

Here are two cases that demonstrate the discovery of aortic aneurysms through careful and complete physical examination and via radiographic studies obtained to evaluate other conditions.

A 51-year-old man with a history of type B aortic dissection presented with severe right upper quadrant pain. He was febrile and hypotensive.

A 69-year-old woman was hospitalized with fever, chills, and nausea. Three weeks earlier, she had received a 2-week course of oral levofloxacin for pneumonia, which resolved. Her history included rheumatic heart disease; diabetes mellitus; depression; a hysterectomy; 2 mitral commissurotomies; nonrepairable mitral valve regurgitation, for which she received a St Jude Medical bileaflet valve; a left-sided cerebrovascular accident; and paroxysmal atrial fibrillation. Her medications included verapamil, furosemide, metoprolol, potassium chloride, metformin, nortriptyline, and warfarin. She denied tobacco and alcohol use.
ABSTRACT: The rate at which acute dyspnea develops can point to its cause. A sudden onset strongly suggests pneumothorax (especially in a young, otherwise healthy patient) or pulmonary embolism (particularly in an immobilized patient). More gradual development of breathlessness indicates pulmonary infection, asthma, pulmonary edema, or neurologic or muscular disease. A chest film best identifies the cause of acute dyspnea; it can reveal pneumothorax, infiltrates, and edema. Pulmonary embolism is suggested by a sudden exacerbation of dyspnea, increased ventilation, and a drop in PaCO2. A normal chest radiograph reinforces the diagnosis of pulmonary embolism, which can frequently be confirmed by a spiral CT scan of the chest. Pneumonia can be difficult to distinguish from pulmonary edema. In this setting, bronchoalveolar lavage and identification of the infectious organism may be necessary to differentiate between the 2 disorders.
Coronary heart disease (CHD) is a significant cause of death in patients with a history of isch- emic stroke or transient ischemic attack (TIA). These patients may have no symptoms of CHD, yet they often have cardiac risk factors.
Severe abdominal pain radiating to the back prompted a 72-year-old man to go to the emergency department (ED). The patient had experienced similar pain 2 days earlier and was treated at another hospital for renal colic on the basis of concomitant microscopic hematuria. He had a history of poorly controlled hypertension.
Painful blue toes developed in a 72-year-old woman with coronary artery andperipheral vascular disease after she underwent angiography.
ABSTRACT: Thrombolysis with intravenous tissue plasminogen activator (tPA), administered within 3 hours of symptom onset, is the only FDA-approved treatment for acute ischemic stroke. Recently, intra-arterial prourokinase was found to improve recanalization and clinical outcome when administered to select patients up to 6 hours after symptom onset. Combination intravenous/intra-arterial thrombolysis can compensate for the delays that are often associated with intra-arterial therapy (products of the paucity of qualified centers and the time required for angiography). Increased risk of hemorrhagic transformation is associated with all routes of thrombolytic administration. However, greater awareness of specific risk factors for hemorrhagic transformation-especially newer CT and MRI criteria-may enable physicians to select patients with an optimal chance of benefiting from thrombolytic therapy, and may also extend the therapeutic window. Despite the higher rate of hemorrhagic transformation, thrombolytic therapy has demonstrated a significant benefit in the treatment of patients with acute stroke.
Currently, the only approved therapy for acute ischemic stroke is tissue plasminogen activator (tPA), initiated within 3 hours of stroke onset. New patient selection criteria are emerging that may improve the effectiveness and safety of thrombolysis. For example, evidence of extensive early ischemia on CT may predict a poor outcome regardless of whether tPA is administered. New imaging techniques, such as diffusion MRI, perfusion MRI, and MR angiography, may be able to identify salvageable tissue and distinguish it from irreversibly damaged tissue. Such findings may allow the 3-hour window for tPA therapy to be extended in certain patients. Other approaches to ischemic stroke therapy that are being studied include intra-arterial thrombolysis, new thrombolytic agents, platelet aggregation inhibitors, endovascular interventional techniques (alone and in combination with pharmacologic thrombolysis), and neuroprotective therapy with various agents to ameliorate the consequences of ischemia in brain tissue.
A 75-year-old obese woman with subacute-onset dyspnea and lower right posterior chest pain was brought to the emergency department. She had a history of diastolic heart failure, arthritis, and suspected obstructive sleep apnea. The patient was dyspneic at rest.
Advertisement
Advertisement
Trending on Patient Care Online
1
GLP-1 Insurance Barriers Are Reshaping OSA Diagnostic Referral Patterns
2
Reishi Mushroom Extract Outperformed Melatonin for Chronic Insomnia in New Study
3
Interpreting Smartwatch Sleep Metrics in Menopausal Patients, With Fiona Baker, PhD
4
Understanding Wearables and Sleep Quality in Chronic Sleep Disorders, With Leanne Kaye, PhD, MPH
5