

























































































































































This year's influenza season is approaching fast. Although the World Health Organization officially declared an end to the 2009 H1N1 influenza pandemic in August, the H1N1 virus is still circulating and is likely to continue to cause serious disease in infants, young children, pregnant women, and other high-risk groups.
Obesity Medicine
Latest News
Advertisement
Advertisement

This year’s influenza season is approaching fast. Although the World Health Organization officially declared an end to the 2009 H1N1 influenza pandemic in August, the H1N1 virus is still circulating and is likely to continue to cause serious disease in infants, young children, pregnant women, and other high-risk groups.

For the past year, a 52-year-old man had dysphagia, which he described as a “knot stuck in the throat” and an associated 25-lb weight loss. He denied fever, chills, headache, abdominal pain, and diarrhea. The patient had been living in the Dominican Republic until about 1 year earlier, when he moved to the United States. He had a 30 pack-year smoking history; he also had hypertension, asthma, and coronary artery disease (none of which were pharmacologically treated). He denied alcohol and illicit drug use.
Quality health measures monitored by insurers include body mass index (BMI), smoking status, and pain.
Your patient is a previously sedentary, overweight 39-year-old woman who has recently taken up running. She now presents with pain and swelling anteroinferior to the lateral malleolus after she twisted her ankle while running on uneven pavement 1 day earlier. Your diagnosis: an uncomplicated lateral ankle sprain.
Here Dr Scheinfeld provides a pictorial guide to neurotic excoriation, perforating folliculitis, chondrodermatitis nodularis chronica helicis, hyperkeratosis, and intertrigo.

Weekend athletes who push themselves too hard can end up with a traumatic or overuse injury that may sideline them for weeks or months-or even permanently. And injury-associated inactivity may result in weight gain and other adverse health effects.
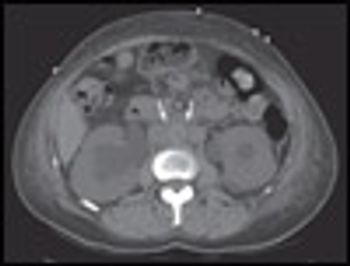
For about 2 weeks, a 61-year-old woman with diet-controlled diabetes and hypertension had fatigue and generalized weakness. For the past 3 months, she had had poorly localized back pain and bilateral flank pain. She denied dysuria, fever, decreased urinary output, or weight loss.

An obese 60-year-old woman presents with a chronic malodorous, itchy rash in her groin.
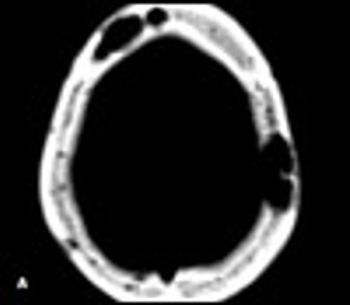
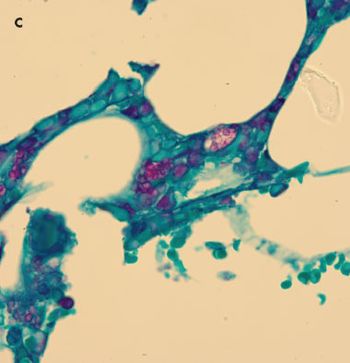
A39-year-old man with a history of AIDS and nonadherence to highly active antiretroviral therapy (HAART) presented with frontal headache and scalp pain of 2 weeks' duration. These symptoms were accompanied by nausea, weight loss, and generalized weakness. Physical examination revealed a small, tender scalp lump, 2 × 2 cm over the left parietal area. The findings from the rest of the examination were unremarkable.
A 3-year-old boy was brought into the office for vague abdominal pain of 5 days’ duration. His mother stated that he had had several episodes of nonspecific pain in the abdomen that lasted a few minutes and resolved spontaneously.
Because epidermal integrity decreases with age, eczematous inflammatory dermatoses are more common among older adults than among younger persons.

A 56-year-old woman seen during physician’s hospice visit. Stormy course from lupus nephritis, dialysisdependency, repeated episodes of dialysis-catheter–related peritonitis, each treated and followed by Clostridium difficile–associated disease.
Dr Rutecki makes some excellent points about the costs of diabetes care and how the reduction of complications such as myocardial infarction, heart failure, and renal disease will decrease costs and suffering. But I have difficulty with the tone of his comments that seem to shift blame for the cause of these costs.
Michael F. Holick, MD, PhD, the Boston University professor of medicine and well-known “apostle of vitamin D,” attracted a standing-room-only crowd Friday for a presentation on his favorite topic. It was a performance that had the audience at rapt attention for a full hour-not just because of the celebrity of the speaker, but because of the extraordinarily clever and engaging nature of his presentation.
Probiotics and prebiotics are now widely used by patients – and even present in many common foods.
I have found that most of my patients with celiac disease actually have to convince their own physicians that they have the disorder.

These grouped, white to flesh-colored papules on the plantar aspect of a 28-year-old woman's heels appeared during weight bearing and disappeared in non–weight-bearing positions. The patient, a nurse whose work required standing for hours, noticed the lesions about a year earlier. Her medical history was unremarkable, and she was taking no medications. Her sister had similar lesions on her heels.
Match the following characteristics with the clinical disorders pictured in the photographs of Cases 1 and 2. Then read the brief descriptions that follow on the next page to see how well you did.
A 58-year-old African American woman comes for a follow-up visit after sustaining a fracture of the right radius, which occurred when she tripped on loose carpeting and broke her fall with an outstretched hand.
What are the long-term effects on the child of maternal health before conception?
For every recognized case of celiac disease, 8 more remain undiagnosed. The reason for this disparity is contingent on the varying presentations of the disease.
American medicine is undergoing the greatest financial scrutiny in its history. The hue and cry for reform stems primarily from the soaring costs of health care. However, placing the blame for these costs solely on increased utilization of technology, cutting-edge pharmaceuticals, cost-shifting hospitals, and physicians misses a bigger mark.
What is the highest dose of insulin that can be used in a patient whose diabetes remains uncontrolled on a regimen of insulin plus an oral antidiabetic agent?
A 38-year-old man had fever and fatigue for the past 6 days and tenderness in the left upper abdominal quadrant for the past 3 days. He also had a facial butterfly rash that had been present for 10 years and a 1-year history of lupus nephritis, treated with prednisone and mycophenolate. He denied respiratory complaints or recent weight loss.
Advertisement
Advertisement
Trending on Patient Care Online
1
Early Liver Disease Detection Starts in Primary Care: A Q&A With Stevan Gonzalez, MD
2
FDA Fast Tracks Remlifanserin Development for Alzheimer Disease Psychosis
3
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
4
ACOG Releases New Guidance on HIV Screening and Prevention
5