
























































































































































An erythematous eruption on the eyelids, asymptomatic papules on the extremities, an acneiform rash--can you identify the disorders pictured here?
Dermatology
Latest News
Advertisement
Advertisement

A 34-year-old woman presented with a blistering, intensely pruritic rash that had erupted 3 days earlier. Multiple papular lesions were densely clustered on areas of exposed skin. Excoriations were present, but there was no evidence of bacterial infection.

For 6 months, a 19-year-old woman had had sensitivity to cold. When outside in cold weather, she noticed swelling, erythema, and pruritus of her uncovered hands. After she held a cold drink on her arm for about 5 minutes, urticarial lesions developed on the skin in contact with the drink. The symptoms resolved about 20 minutes after the cold source was removed. She denied angioedema, respiratory symptoms, light-headedness, and tachycardia.

These pinpoint pustules, some with excoriations, and surrounding erythema appeared on the posterior trunk and outer arms of a 15-year-old boy after he had wrapped his upper body in a wool blanket. These lesions were occasionally pruritic, especially on the arms, where most of the excoriations were noted.

This black lesion had been present on the upper back of a 5-year-old girl since birth. The lesion had gradually enlarged to its current size of 1.5 cm. In the past year, 3 satellite black macules had developed in the surrounding area.
Lines of Blashko may represent normal embryonic movements of the skin during embryogenesis.
This 11-year-old boy has a segmental café au lait macule in a zosteriform distribution. Because the presence of such a lesion may signify somatic mosaicism, a careful review of systems and physical examination of affected patients is indicated. The same cautions apply to patients with large (10-cm) café au lait macules. This patient is vigorously healthy.
McCune-Albright syndrome is classically described as a triad of polyostotic fibrous dysplasia, café au lait macules, and precocious puberty. The syndrome may also be accompanied by various other endocrinopathies including hyperthyroidism, acromegaly, hyperprolactinemia, Cushing syndrome, and hypophosphatemic rickets. Some patients may also exhibit hepatic, cardiac, and GI dysfunction.
This 4-year-old boy has urticaria pigmentosa--one of a group of disorders in which mast cells group together in the skin. Patients may have solitary mastocytomas or (rarely) diffuse infiltration of the skin with mast cells.
This is an autosomal recessive syndrome characterized by chromosomal breakage, pancytopenia, and various congenital abnormalities. It is a heterogeneous condition clinically and has been linked to defects in at least 8 different genes. Fifty percent to 65% of affected persons demonstrate areas of hyper- or hypopigmentation. Café au lait macules, like those shown in Figure A in a 9-year-old boy, are seen in approximately 25% of those affected.
The 12-year-old boy in Figure A has one large and one small café au lait macule and a single hypopigmented macule. Solitary café au lait macules may be present in as many as 30% of newborns. They vary in size from a few millimeters to several centimeters. The macules may be inconspicuous until the affected area is exposed to the sun.
A 14-year-old African American boy presented during the winter months with a painless, nonpruritic, periumbilical rash that had been present for approximately 1 month. Initially bluish, the rash had become dark brown.
A collage of hyperpigmented macules.
Skin signs of systemic disease: sarcoidosis, rheumatoid nodules, Muir-Torre syndrome, diabetic vasculopathy, hyperlipidemic nodules, zinc deficiency, and Sister Mary Joseph nodule.
Solitary intraductal papillomas are tumors of the major lactiferous ducts. They occur most frequently in women 30 to 40 years of age, and frequently present with nipple discharge.

An enlarging mass was noted on the dorsum of the right fifth toe of a 2-month-old boy during a well-child examination. The firm, immobile mass measured approximately 1 cm in diameter. A congenital abnormality was suspected; the patient was referred to a plastic surgeon for consultation.
A 51-year-old man presented with red, mildly pruritic papulonodules that had erupted on his face approximately 5 weeks earlier. The clinical appearance suggested cutaneous lymphoid hyperplasia.
Sclerosing adenosis most commonly occurs as multiple microscopic foci, although occasionally it presents as a palpable mass.
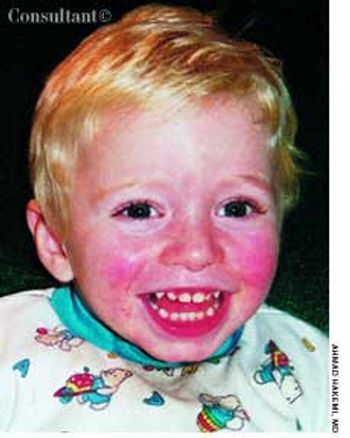
The parents of a 2-year-old sought treatment for a rash on their son's face. The child had had a low-grade fever for 3 days before the rash erupted. An intermittent lace-like rash was beginning to develop on the extremities. The patient was otherwise asymptomatic.

A 17-year-old girl sought evaluation of multiple face and neck nevi. The lesions had been present at birth and were becoming darker as the teen grew older. She reported no family or personal history of skin cancer or dysplastic nevi.

Identical circular, chocolate-colored spots developed on a 4-year-old boy's palms 2 weeks ago, according to the child's mother. The sharply demarcated, macular lesions were asymptomatic.

An 83-year-old man with a history of hypertension and coronary artery disease presented with a 4-day history of mental status changes, slurred speech, and difficulty ambulating. He reported a lack of appetite and weakness of several days.

Extremely itchy, crusting nodules appeared on the arms and legs of a 42-year-old woman who was undergoing renal dialysis.

A painless swelling on the dorsum of the scalp had been present for many years in a 36-year-old man. An increase in the size of the lesion prompted the man to seek medical evaluation.

Cutaneous manifestations develop in approximately 30% of persons with diabetes. Premature atherosclerosis is a common complication of the disease that can cause peripheral infarction, ulceration, and necrosis.
Advertisement
Advertisement
Trending on Patient Care Online
1
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
2
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
3
ACOG Releases New Guidance on HIV Screening and Prevention
4
Compulsive Smartphone Use Linked to Depressive Symptoms in Older Adults
5