




























































































































































Progressive weakness and fatigue for the past 6 months prompted a 43-year-old woman to consult her physician. She denied diarrhea, melena, hematochezia, cough, fever, and night sweats. Her skin and conjunctivae were pale.
Progressive weakness and fatigue for the past 6 months prompted a 43-year-old woman to consult her physician. She denied diarrhea, melena, hematochezia, cough, fever, and night sweats. Her skin and conjunctivae were pale.

Consider this diagnosis when a patient presents with a history of rapid, diffuse hair loss. Telogen effluvium affects the entire scalp, but the crown and bitemporal areas may appear to be mainly involved if there is associated androgenetic alopecia.

This rare condition affects both men and women. The average age at onset is 53 years. The lesions are deep brownish red to purple papules, nodules, and plaques. Blisters and ulcers also can occur.

A 72-year-old morbidly obese man who had diabetes mellitus was admitted to the hospital from a nursing home with a fever of 4 days' duration. A tracheostomy had been performed 3 months earlier for respiratory failure. The patient was being treated with corticosteroids for chronic obstructive pulmonary disease.

A 44-year-old man sought relief from severe pain, swelling, and restricted radiocarpal and digital motion of his left hand. Four months before, he had suffered a fracture of the distal radius metaphysis (Colles' fracture), which was treated by closed reduction with long-arm cast immobilization for 6 weeks.

A 38-year-old woman had become increasingly depressed by worsening psoriasis in conjunction with a flare of arthritis in her hands and fingers. The patient complained that she could not function optimally and that her quality of life had diminished.

A 45-year-old man presented with a 2-month history of progressive fatigue, weight loss of 10 lb, abdominal pain, and pruritus. The patient had been taking a maintenance dose of oral mesalamine since he received a diagnosis of ulcerative colitis 14 years before.

The foot of a 10-year-old boy demonstrates the unique wandering cutaneous lesions of creeping eruption, or cutaneous larva migrans. This disorder is caused by skin penetration of hookworm larvae. It is seen in the southeastern United States and tropical and subtropical regions throughout the world.

Encountered rarely these days, scarlet fever is believed to be caused by sensitization to an erythrogenic toxin produced by strains of group A β-hemolytic streptococci. Thus, previous exposure to the toxin is necessary for development of the rash seen here-fine, sandpaper-like, and papular on an erythematous background. It usually begins on the trunk and spreads over the entire body within hours or days. Scarlet fever is unusual in infancy, possibly because of maternal transfer of antibodies.

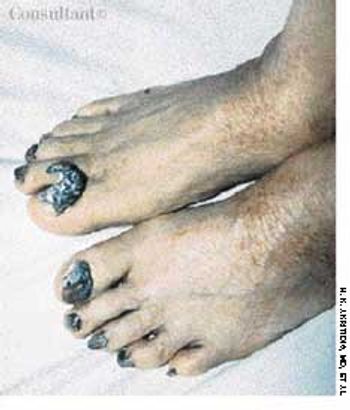
Large, blue-black, macular areas over the buttocks and presacral regions were present at birth in this black child. Significant hyperpigmentation of the genitals also was evident. Scrotal hyperpigmentation is not an uncommon finding in a black newborn. However, the intensity of the penile hyperpigmentation in this baby is unusual.
A 32-year-old construction worker sought evaluation of nontender skin lesions that had been erupting for several months. The patient was seropositive for HIV with a CD4+ cell count of 210/µL. He had no history of opportunistic infections.

The asymptomatic skin lesions seen on this 66-year-old woman had been present for 7 months. Therapy with topical and oral antifungal agents had failed. The annular patches were pale to bright red and very slightly scaly; they affected the lower third of the patient's back and abdomen and her flanks, buttocks, and upper thighs.

Dermatophyte infections have a predilection for certain anatomic sites, such as the feet, groin, and scalp. Tinea corporis refers to involvement of the trunk and extremities. The condition arises either from direct exposure to an infected source or by extension from an adjacent affected site. Itch is a common symptom, but the intensity of the pruritus can vary from patient to patient.

A 39-year-old man who has sickle cell disease suffers with chronic ankle ulcers typical of the disorder. Ulcerations occur in approximately 50% of persons who are homozygous for sickle cell disease.

A new lesion recently arose on the right flexor forearm of a 67-year-old man. The 1-cm, pruritic, pink, circular, slightly raised lesion was perfectly homogeneous with no central clearing.

A 36-year-old man was admitted to the hospital with acute mid-epigastric pain and vomiting. He was a heavy drinker and had smoked between 50 and 60 cigarettes a day for the last 15 years.
This patient, a woman, presented with onychogryphosis, a severe nail change seen on the toes, especially the great toe. Thickening and hardening of the nail substance with a curved growth pattern produces this abnormal clawlike configuration.

Eczema was the original diagnosis of this pink, scaly, asymptomatic patch on a 44-year-old man's chest. A mid-potency corticosteroid ointment had been prescribed but had no effect on the lesion. Now, 18 months later, the patient said the patch had been slowly enlarging.
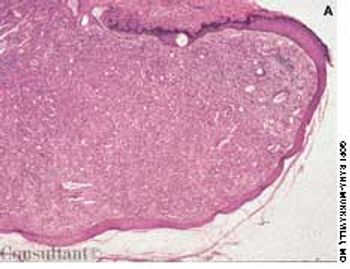
These benign tumors made up of nevus cells may be flat or raised, pigmented (Figure A) or nonpigmented.

A 67-year-old woman sought medical treatment for the persistent, large “blackheads” on her face. Examination revealed diffusely thickened and yellowed skin with deep furrows. The periorbital and malar areas were studded with large open comedones.

Pruritic urticarial papules and plaques of pregnancy (PUPPP). This cutaneous eruption usually occurs in the last trimester. It is seen only rarely in the postpartum period. PUPPP is more common in primigravidas but can occur in any pregnant patient.

After 6 months of suffering with an infection on her finger and several failed courses of antibiotic therapy, a 53-year-old woman sought a second opinion.

A 60-year-old man presented with redness, swelling, and pain on his right lower leg of 3 day's duration. He recalled being scratched by underbrush while hiking in the woods a few days earlier; the patient denied other recent trauma or insect bites.

A 71-year-old man, who had recently returned from a month in Europe, complained of left lower leg swelling and pain of 1-week's duration. For many years, this obese patient had chronic venous insufficiency of both legs and chronic osteoarthritis of the knees that severely limited his ability to walk. The patient was admitted to the hospital with extensive cellulitis of the left lower leg.
For 6 years, a 32-year-old man had a recurring rash on his back, shoulders, and chest. He stated that the rash appears in the spring, itches, and enlarges into ringlike areas. Previously, when treated with cephalexin, the rash had cleared within several weeks. Antifungal medication (econazole cream and oral terbinafine) had failed to resolve the rash.