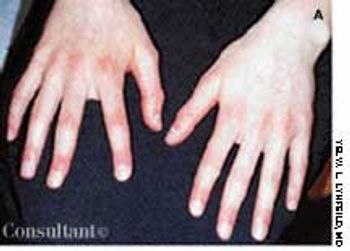





























































































































































Seen here are a 38-year-old Native American woman and her 20-year-old daughter, each of whom has had a relapsing eruption for several years. Pruritic, red to red-brown plaques develop on their faces and necks and on the dorsal surface of their hands. Scattered brown and hypopigmented macules as well as some scaling and slight erythema appear on their lower lips. The women stated that the eruptions flare each spring and gradually improve throughout the rest of the year. The daughter's lesions were more acute at this time and had developed during the preceding 3 days.