






























































































































































A 66-year-old man presented with numerous cutaneous tumors. He had dementia and thus was unable to provide an accurate history.
A 66-year-old man presented with numerous cutaneous tumors. He had dementia and thus was unable to provide an accurate history.

This asymptomatic lesion on the upper arm of a 60-year-old man had been present for 2 years. The patient had used several over-the-counter antifungal and hydrocortisone creams to treat what he thought was ringworm.

For 3 years, a 53-year-old man had noted increasingly extensive changes in his skin, including facial thickening, a progressive reddish tinge, and annular lesions on his trunk. He also complained of itching on the periphery of his face.
Exquisite pain of 3-days' duration in his right index finger sent a 19-year-old man for medical consultation. He recalled that a thorn had become embedded in the finger while gardening 1 week earlier.

A 68-year-old woman was referred from an acute care clinic for evaluation of a persistent cellulitis. Ten days before, erythematous, pruritic plaques developed on her ankles; these slowly enlarged, and pustules formed. The patient denied fever or chills. Her past medical history was unremarkable, and conjugated estrogen, medroxyprogesterone acetate tablets, and multivitamins were the only medications and nutritional supplements she was taking.

Four months after a patchy, macular, erythematous spot erupted on the dorsum of a 63-year-old woman's left foot, the area became ulcerated, tender, and painful. The 1.2-cm ulcer was covered by a hemorrhagic crust surrounded by a cyanotic reticular discoloration of the skin.

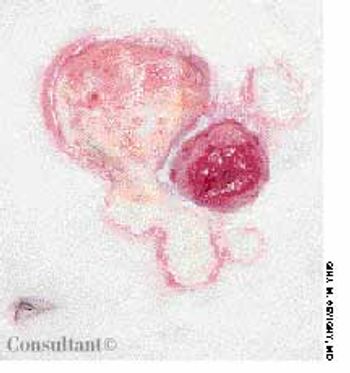
This red papule developed 6 months ago at the base of a 53-year-old woman's thumb. The lesion was asymptomatic, but it bled easily when traumatized. It was treated definitively with surgical excision, and the biopsy report was consistent with the clinical diagnosis of pyogenic granuloma. This most commonly appears on the face or fingers and may result from minor trauma.
A painful skin eruption surrounding her colostomy stoma had appeared several months ago and was slowly increasing in size, complained a 64-year-old woman with Crohn's disease. The lesion consisted of several coalescent ulcers with a yellow, fibrinoid base and a violaceous, undermined border.

A 42-year-old woman had had athlete's foot for years, but the condition suddenly worsened when inflamed, pruritic vesicles appeared on both feet. A few days later, tiny, mildly itchy vesicles erupted on her palms; the rest of the hands were not involved. One week after the palmar eruptions, the patient noted 2 round, reddish brown, asymptomatic 3-cm macules on her trunk. These lesions had faint scaling on the trailing edge of the slowly advancing arciform borders.

Five days after beginning aggressive treatment with intravenous corticosteroids for inflammatory bowel disease, this 26-year-old man noticed the sudden eruption of this mildly pruritic rash.

The mother of a 6-year-old boy was concerned because there was a whitish mass between the glans and foreskin of her son's penis. She thought that this might be an accumulation of “pus.”
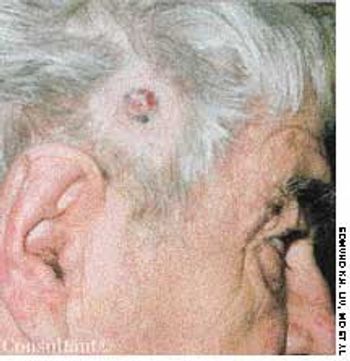
A 67-year-old man had been aware of a painless, firm, red nodule that had been growing slowly on the right temporal area for 1 year. The lesion occasionally bled.

A 76-year-old woman had a 40-year history of rheumatoid arthritis (RA). She had repeatedly refused treatment with disease-modifying drugs, including methotrexate. Nodules began to develop 15 years after the initial diagnosis; they recurred after surgical removal.

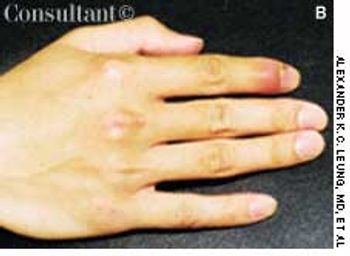
A 65-year-old woman, who was confined to a wheelchair because of severe rheumatoid arthritis, was concerned about nodules that had erupted on her fingers and hands during the previous 3 weeks. Her medical history included colon cancer, chronic renal insufficiency, anemia, and hypertension. The nonpruritic nodules were painful when they began to form under the skin; however, once they erupted, the pain disappeared.

A variety of rheumatic diseases-systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and the vasculitides among them-manifest as “lumps, bumps, and holes” involving the extremities. Each of these diseases works through specific mechanisms on different structures of the skin to produce a distinctive pathology. In doing so, each provides clues to the cause, which the history and physical examination can help confirm.

This 64-year-old woman has had rheumatoid arthritis for 15 years; her hands show classic rheumatic changes. She also had a leg ulcer that had failed to heal in 8 years despite three skin grafts.

Various types of cutaneous lesions may occur in association with RA, including rheumatoid nodules, rheumatoid neutrophilic dermatitis, vasculitis, palpable purpura, and pyoderma gangrenosum. Many of these manifestations-including rheumatoid nodules-are specific for RA. The presence of these nodules is associated with seropositive disease and with a more severe, erosive clinical presentation. The nodules appear in 20% to 30% of patients with RA. Sites of predilection are those subject to shear stress, including the subcutaneous tissues over the extensor aspects of the elbow region, over the sacrum in bedridden persons, and at the pericardial and pleural surfaces.

Cutaneous and subcutaneous lesions of the extremities may be clues to the presence of rheumatic diseases such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and the vasculitides. The history and physical examination can generally help confirm the cause. Skin biopsy is sometimes necessary for a definitive diagnosis; useful results depend on a technique that gives the depth necessary to see the pathology and proper interpretation of biopsy specimens by an experienced dermatopathologist.

Pyoderma gangrenosum (PG) is a chronic, recurrent condition characterized by cutaneous ulceration. In half of patients, PG is associated with an underlying illness, such as inflammatory bowel disease, RA, SLE, or a lymphoproliferative disorder.

This 20-month-old girl was born to a 28-year-old mother at 38 weeks' gestation. The pregnancy was uncomplicated, and vaginal delivery was normal. The infant sat with support at 10 months of age, sat without support at 12 months, crawled at 13 months, and walked at 18 months. She had not yet begun to talk at 20 months. The child was noted to have frequent laughing episodes and often made flapping movements with her hands.

A 29-year-old man presented with a complaint of venereal warts and a long history of mild psoriasis, which he had treated with fluocinolone. He returned 3 months later complaining of chest congestion of 10 days' duration; it had been treated with ciprofloxacin at an urgent care facility.

Loss of pigmentation is noted around the left eye of a 49-year-old African-American man-the same eye in which he has a detached retina. In addition, the patient's hearing is impaired on that side.

A 68-year-old man presented to the emergency department (ED) complaining of an itchy rash over his body. His past medical history included hypertension, contact dermatitis, and penicillin allergy.

Highly pruritic, 2- to 4-mm, papular lesions with central ulceration erupted on the back of a 66-year-old woman. She had had 2 similar outbreaks in the past. The patient was taking conjugated estrogens, alprazolam, and alendronate.

A 43-year-old woman requested removal of a lesion from her left axilla because it had recently become irritated. The polypoid lesion with dried terminal ulceration had been present for 17 years.