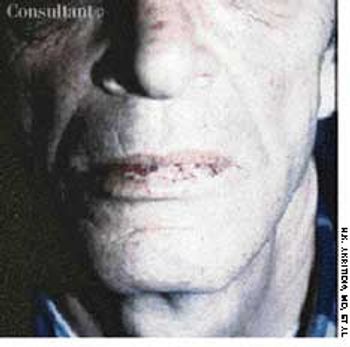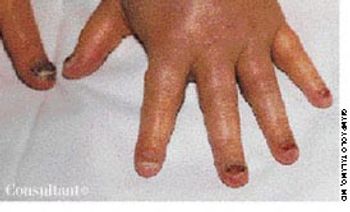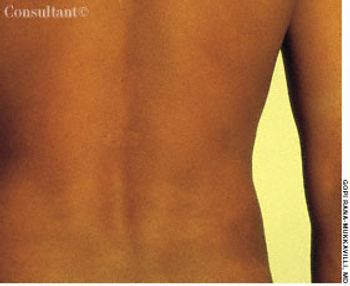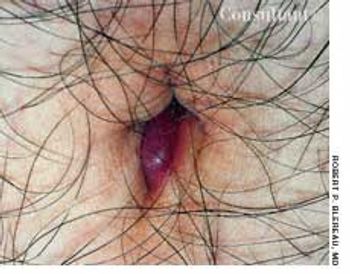
A comatose 29-year-old woman was brought to the emergency department. Her family reported that she had been well until 4 days earlier, when headache and fever developed. She went to another hospital at that time and was told she had an abscessed tooth. She was given erythromycin, and the tooth was extracted the following day. The patient's headache and fever worsened; a sore throat also developed, and a rash appeared on her trunk, arms, and legs. The family denied any HIV risk factors, unusual medical history, recent travel, and exposure to persons with infectious diseases.