





























































































































































This 7-year-old presented with a pink, raised lesion on her upper left eyelid. The 1-cm lesion contained tiny vesicles and showed eccentric central clearing.
This 7-year-old presented with a pink, raised lesion on her upper left eyelid. The 1-cm lesion contained tiny vesicles and showed eccentric central clearing.

Seen here is an ulcerated tumor with irregular borders on the left foot of a 37-year-old man. He said the tumor had developed several years ago.

Ten days after ballet practice, a 9-year-old girl noticed a nonpruritic, petechial rash on her lower legs. Swelling of the ankles and knees was also apparent. The patient was afebrile, otherwise healthy, and had no abdominal pain. There was no family history of blood dyscrasias. The patient was taking no medications.

For more than 20 years, a 55-year-old man had a faintly erythematous, papulosquamous rash with arciform borders on his groin and waistline. The rash had been treated with a variety of medications. Topical and oral antifungals and antibiotics and topical corticosteroids had been used but to no avail. No laboratory tests had been performed.
Flat, tan-pink patches on his lower legs disturbed a 52-year-old man. The lesions had visible, nonpalpable petechiae, which did not blanch on diascopy; telangiectasia and inflammatory vasodilation, therefore, were excluded from consideration.

A 51-year-old woman with severe migraines sought evaluation of a dozen round black macules on her hands, forearms, and legs. A few of the lesions had first appeared 1 year earlier; the remainder had erupted since then.

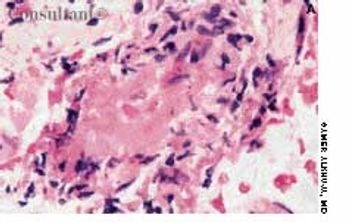
Flesh-colored to red-brown nonpruritic papules developed most prominently on the elbows, forearms, and knees of a 2 1⁄2-year-old boy. The rash was preceded by a low-grade fever and mild, upper respiratory tract symptoms.

A 46-year-old man complained of “irritation” in the groin of several months' duration.
A 67-year-old man was concerned that the peeling lesion near his eyebrow was cancer.
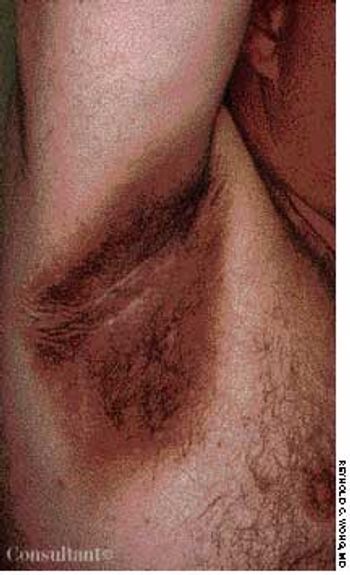
Brown-black discoloration and a soft, velvety papillomatosis of the axillary, inguinal, genital, and neck areas were seen in a 46-year-old man. He had hypertriglyceridemia, for which he had recently begun taking nicotinic acid. After a few days of therapy, he noticed the onset of this asymptomatic hyperpigmentation.
These lesions are always present at birth. They consist of mature dilated capillaries and represent a permanent developmental defect. They are red to purple, macular, and sharply circumscribed. They are usually unilateral and may occur anywhere on the body, although they tend to favor the face. Unlike salmon patches, port-wine stains do not fade; in fact, they tend to darken and become nodular with age.

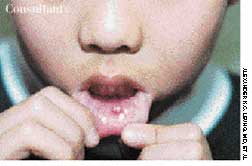
For 2 days, an 80-year-old woman had left ear pain and a rash around the ear canal and pinna. She also complained of pain and small papules in the back of her pharynx on the left side. She had no fever or chills and no rash elsewhere on her body. She denied drainage from the ear and previous ear infections or skin eruptions. Several years earlier, she had undergone surgery and chemotherapy for lymphoma but had been well since then.

A 75-year-old Hispanic woman presented with a slowly growing, asymptomatic facial lesion of about 3 years' duration.
Gross cysts (palpable fluid-filled macrocysts) are the most common lumps found in the breast. Cysts vary tremendously in size and number and may be microscopic or macroscopic.

A 21-year-old man slept in a car in upstate New York for three winter nights. Discomfort and swelling of his toes developed, which progressed to marked discoloration of the digits.

A 69-year-old woman, who was being seen regularly for treatment of psoriasis, was noted to have numerous open comedones on the sides of her face in association with photodamaged skin.

After having been bothered by these lesions for the past 9 months, a 27-year-old woman described the eruption as "itchy bumps under my arms."
Worsening episodes of pain and bleeding from the lesion on the dorsum of her foot brought a 16-year-old girl to her physician's office. The spot had gradually enlarged since she first noticed it about 3 years earlier.

A 23-year-old man complained of unsightly “flat warts” all over his chest. These lesions first appeared in early adolescence. The clinical suspicion of epidermodysplasia verruciformis was confirmed by a biopsy.

A 61-year-old man with a history of squamous cell carcinoma was concerned about a tender nodule on his ear. He complained of exquisite tenderness with pressure, such as when lying on the affected side at night.
Following two witnessed tonic-clonic seizures, a 65-year-old woman with a history of chronic obstructive pulmonary disease was admitted to the hospital. Results of laboratory studies included serum creatinine level, 2 mg/dL; blood urea nitrogen level, 28 mg/dL; and erythrocyte sedimentation rate, 61 mm/h. The patient's antinuclear antibody (ANA) titer was 1:40 with a speckled pattern, and creatinine clearance was 17 mL/min. An ultrasonogram revealed bilateral small kidneys. CT and MRI of the head revealed no abnormalities.

For 2 months, a 22-year-old uncircumcised man noticed an asymptomatic, erythematous, static lesion on the glans penis. He had applied an over-the-counter “jock-itch” ointment for 2 weeks but to no avail. The young man was otherwise healthy and denied having dysuria or a history of sexually transmitted disease.

A 24-year-old man presented for evaluation of pruritic vesicles on both feet. Ten days earlier, dyshidrotic eczema had been diagnosed by another physician who prescribed triamcinolone ointment. The patient reported that the foot eruption worsened after the topical medication was applied.

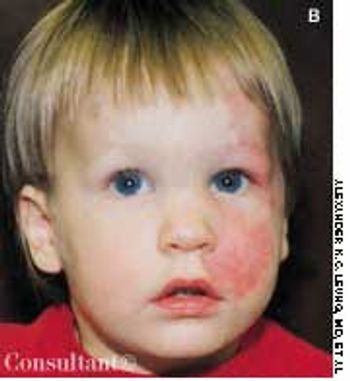
This 6-year-old boy was brought to his physician for evaluation of a rash. The child had been running a fever and, for the past 48 hours, had been complaining of a sore throat, headache, and abdominal pain.
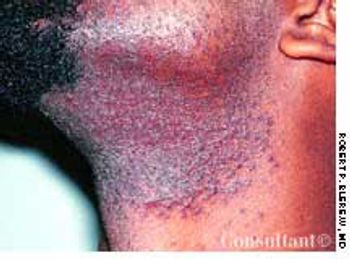
The rash on the neck of this 24-year-old man first appeared when he began to shave as a teenager. Pseudofolliculitis barbae affects 50% to 75% of black persons and 3% to 5% of white persons who shave.