





























































































































































A 6-year-old boy presented with a painless, bluish swelling in the superotemporal orbital quadrant (A) that had been enlarging since infancy.
A 6-year-old boy presented with a painless, bluish swelling in the superotemporal orbital quadrant (A) that had been enlarging since infancy.
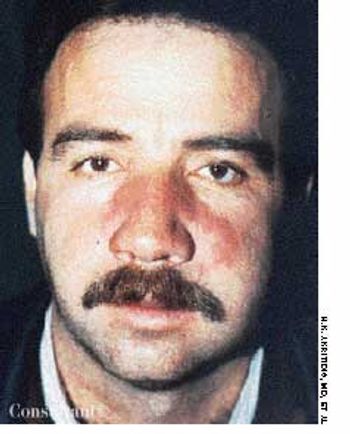
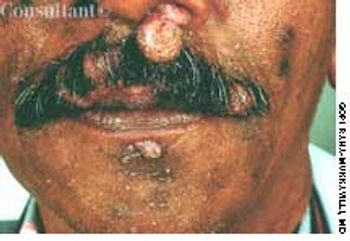
A 40-year-old man was hospitalized with the superficial, reddening, and painful facial lesion seen here. Its borders were sharp, and it had developed rapidly. The patient had a temperature of 40°C (104°F) and chills. His erythrocyte sedimentation rate was elevated, and he had neutrophilic leukocytosis.
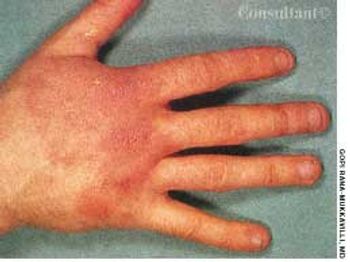
After 1 week of scratching a pruritic, reddish rash on a swollen hand and enduring a “burning sensation,” a 43-year-old man visited his physician. The patient worked as a meatpacker. He had no other medical conditions, took no medications, and had no known drug allergies.

A 68-year-old man presented with a sudden-onset, 2.5 × 2-cm, rock-hard, erythematous, nontender nodule on the right side of the chest. A dense mat of telangiectases surrounded the solitary lesion. The remainder of the cutaneous examination was unremarkable.

Tortuous, dilated varicosities; multiple smaller caliber abnormal perforating vessels; and chronic brawny edema of chronic venous insufficiency (CVI) were seen on a 70-year-old man's left leg. He reported that the edema and discoloration had worsened over the last 15 years. The brawny edema stopped just above the ankle, indicating that compression by the patient's sock controlled the signs and symptoms of CVI.

A 60-year-old woman was referred by her gynecologist because of a lesion on the buttocks of which the patient first became aware when she noticed blood on her underwear. Physical examination revealed an irregularly pigmented and slightly eroded asymmetric plaque. Examination with a magnifier highlighted a slightly rolled border, from which a shave biopsy was performed.

After more than 15 years of wondering what the “white specks” on his legs were, a 64-year-old man consulted his physician. The patient was taking medication to control hypertension; he was otherwise healthy.

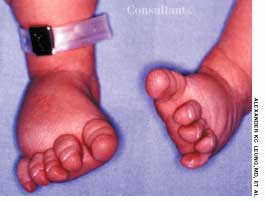
Following an uncomplicated pregnancy, a 30-year-old gravida 2, para 1 mother delivered a term infant boy. The neonate's Apgar scores were 7 at 1 minute and 9 at 5 minutes. Birth weight was 3.2 kg (7.1 lb); length, 50 cm (19.7 in).

Erythematous, scaly lesions with double-edged borders had been present on a 14-year-old boy's left upper arm and lower legs for about a year. The lesions were occasionally pruritic, and some resembled ringworm. At times, fine yellow crusting suggestive of impetigo was present. The boy took very hot baths and showers.

An eruption on the face of a 49-year-old woman had been misdiagnosed as a staphylococcal infection; the rash failed to respond to oral and topical antibiotics. A mid-potency topical corticosteroid also had been tried, but the eruption worsened.

Mongolian spots are benign, congenital blue-gray macules or patches commonly found in Asian, black, and Hispanic infants (and in 5% of white infants). They are most often located in the sacrogluteal area and the upper back. The lesions may be solitary or multiple, vary in color intensity, and frequently enlarge until about age 2, when they gradually fade and disappear. Approximately 5% persist into adulthood.

The widespread eruption of asymptomatic macules and flat, palpable, flesh-colored lesions prompted a 23-year-old woman to consult her physician. The lesions-some of which had dark centers-were concentrated on the patient's face, neck, and upper back; the palms, soles, anal mucosa, and genital areas were clear. The patient denied systemic symptoms. She was seronegative for HIV.

A papule on the leg of an 11-year-old boy had suddenly developed into a slightly tender pustule. The pustule had not responded to oral cephalexin and topical mupirocin prescribed by another clinician.

Cutaneous photosensitivity followed by acute, then chronic, skin lesions on sun-exposed areas characterizes this disorder.

The significant palmar erythema seen on the hands of a 60-year-old man with alcoholic cirrhosis is a sign of underlying chronic liver failure.

Two 7-year-olds show the purpuric rash of the lower body and legs that is typical of Henoch-Schönlein purpura. This disease is a vasculitis that chiefly affects small vessels of the skin, joints, gastrointestinal tract, and kidney.

A 3-mm long, double-tipped, polypoid lesion appeared just anterior to the anus on an 8-month-old girl 2 days earlier. The lesion was excised in the office: a local anesthetic was administered, and the base was lightly electrodesiccated. Antibiotic ointment was applied until the area healed. Pathologic findings identified an infantile perianal pyramidal protrusion.

A 52-year-old white man presented with a pruritic eruption on the neck of 3 months' duration. The rash had not responded to a potent topical corticosteroid prescribed by another practitioner for the presumed diagnosis of eczema.

A 13-year-old girl who had leukemia presented to the emergency department with fever; chills; weight loss; fatigue; and a painful, erythematous rash with a central black lesion on the upper thigh. The patient was neutropenic and had been undergoing chemotherapy for 1 week.

A healthy 31-year-old man was referred to a dermatologist with a diagnosis of tinea versicolor that did not respond to oral ketoconazole and topical selenium sulfide.

The entire scalp of this 1-month-old boy shows the diffuse yellow scaling of seborrheic dermatitis. Called “cradle cap” in infants, this dermatitis typically begins on the scalp during the first 3 months and may spread over the entire face. An associated stubborn diaper rash may develop in some infants.

A 70-year-old man was concerned about these dark lesions that covered his back and legs.

Shortly after arriving from Puerto Rico, a 59-year-old man presented with right-sided frontal head pain and decreased vision in his right eye. He was concerned about a “sore” that first developed 9 months earlier on his head. The patient denied fever, chills, and syncope.
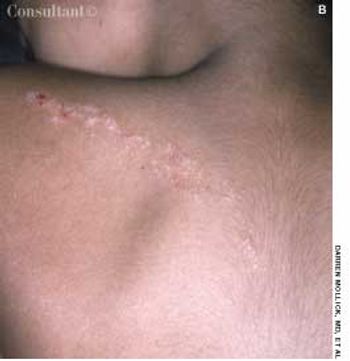
A 7-year-old boy with a history of atopic dermatitis presented with an intensely pruritic linear rash on his upper extremity. His mother reports that the rash has been “growing” despite use of topical corticosteroid creams.
A 57-year-old man who had recently arrived in the United States from El Salvador presented with a nodular growth in his left naris. He reported that the lesion, which had been slowly progressing for several months, now completely blocked his left nostril. His only symptom was impaired inhalation.