























































































































































The mother of a 6-year-old child brings her to your office becauseof a pruritic rash that has been present for several days. The rash did not respondto hydrocortisone cream and has continued to spread along the patient’sleft side.
Dermatology
Latest News

Advertisement
Advertisement
My patient is a 42-year-old woman who experienced a nonblanching, purpuricrash and edema of the lower legs after she started taking nifedipine (Figure).

A 32-year-old man who was seropositive for HIV presented with a tender lesion on his right foot of about 3 months' duration. The patient's only medication was zidovudine. His CD4+ cell count was 120/µL.

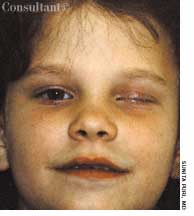
For 1 month, a 25-year-old woman had experienced discomfort in and around the left eye and diplopia. She was in good health; she reported no weight loss, excessive nervousness, heat intolerance, decreased strength, changes in the texture of hair or skin, or altered bowel habits. There was no personal or family history of goiter or other thyroid disease.

A pruritic rash developed on the feet of a 40-year-old woman 2 days after she had worn a new pair of shoes for a few hours. The erythematous, papular, scaly eruption was more prominent on the right foot.
For 2 days, a 43-year-old woman has had a slightly tender rash on her trunk andextremities. Five days earlier, the patient was given levofloxacin for an upperrespiratory tract infection; because she is prone to yeast infections while takingantibiotics, fluconazole also was prescribed.
A previously healthy elderly woman reports that she has hadunilateral facial pain and crusting skin lesions for several days. She decides toseek medical care because of concomitant impaired visual acuity.
Several of my female patients have chronic itchy, burningvulvitis.
A 75-year-old woman complained of“tired and heavy eyes” and being unableto keep her eyelids open to readat night.

Incarcerated umbilical herniations occur through the umbilical canal that is bordered by the umbilical fascia posteriorly, the linea alba anteriorly, and the medial edges of the 2 rectus sheaths on each side.

A 62-year-old woman presented with a rash and intermittent pain of the right upper quadrant. The reticular, brown hyperpigmentation was also seen on her right flank and around the umbilicus. The patient reported that she often applied heating pads to these areas for pain relief.
A 63-year-old woman seeks evaluation of a persistent, rough, red area onthe dorsum of her left index finger. The lesion has been present for severalmonths. The patient’s manicurist is convinced it is a wart.
A 37-year-old woman complains of “itchy bumps” that erupted just above herwaist 2 or 3 days earlier. She denies having had this condition in the past.The patient is otherwise healthy and takes no medications. An avid gardener,she claims to be able to identify and avoid poisonous plants.
I read with interest Dr Virenda Parikh’s case of a young woman with extensiveanal condylomata acuminata (CONSULTANT, April 15, 2001, page 737).

The mother of this 5-month-old boy was concerned about the large birthmark in the infant's diaper area.
My patient reports that erythemanodosum occurred when she took anoral contraceptive (OC) in the1990s.
Some degree of hyperpigmentationdevelops in most pregnantwomen. This coloration is more pronouncedin dark-skinned women; onnaturally pigmented areas, such as theareolae, perineum, and umbilicus; andon the axillae, inner thighs, and otherregions that are prone to friction.
A 24-year-old woman's firstpregnancy was uneventful until thesixth month when mild malaise and ahighly pruritic abdominal rash occurred(Figure 1). A biopsy and directimmunofluorescence confirmedthe suspected diagnosis of herpesgestationis.
Foot ulcerations and infections are the leading cause of hospitalizationamong patients with diabetes; they occur in about15% of these patients. Given the rapidly increasing incidenceof diabetes, physicians can expect to see a growing numberof diabetic foot problems. Here, a group of experts, many ofwhom practice at the renowned Joslin-Beth Israel DeaconessFoot Center in Boston, offer guidance on all aspects of diabeticfoot care. The topics covered range from proven preventivestrategies to cutting-edge wound care techniques that drawon such new developments as growth factors and living skinequivalents. A detailed review of the pathophysiology of thediabetic foot is also included. The emphasis throughout is ona multidisciplinary approach that incorporates the servicesof diabetologists, podiatrists, orthopedic surgeons, orthotists,diabetic nurse educators, and others. Numerous black-and-whiteand color photographs, drawings, algorithms, and charts illustratethe text.
Although many patients with primary HSV-1 infection have no clinicalrecurrences, the failure to seroconvert occurs very seldom-inno more than 1% of patients.
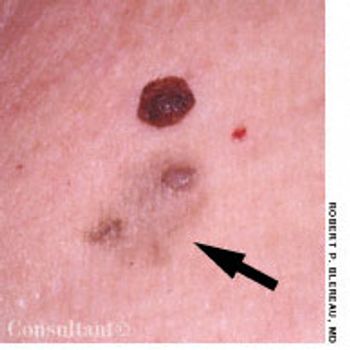
Two asymptomatic lesions that had been present for 1 year on the left upper chest of a 61-year-old man were excised. Pathologic examination revealed the raised, dark brown medial lesion to be an interdermal nevus; the lateral, light tan lesion with papules was a papillomatous interdermal nevus with primary macular amyloidosis.
Match each picture with the phrase below that best describes it. The organisms in these pictures might be microscopicor macroscopic, and they can be recovered from skin lesions or clothing by the patient and/or clinician.
A 72-year-old man slipped and fell backward in the bathroom, hitting hishead on the toilet seat; he suffered only minimal discomfort. The followingday, he presented with mild back pain and extensive bruising.
A middle-aged woman reports that for several days she has hada facial rash, some mild facial discomfort, and a low-grade fever. She deniesprevious illness, recent contacts with infected persons, or history of a similarrash.
For 3 days, a 36-year-old woman has had a painful rash on the dominant lefthand. She had noticed a tingling sensation before the lesions erupted. Thepatient is otherwise healthy and takes no medications. She is a teacher.
Advertisement
Advertisement
Trending on Patient Care Online
1
ACOG Releases New Guidance on HIV Screening and Prevention
2
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
3
2026 Dyslipidemia Guideline Expands Statin Eligibility to 21.5 Million More US Adults
4
FDA Accepts Cefiderocol sNDA for Pediatric Gram-Negative Infections
5