






























































































































































A 63-year-old woman presents withdiffuse hyperkeratosis of the solesand palms. She also has onycholysis-separation of the nail plate fromthe nail bed-and salmon-coloredplaques behind her ears. Biopsy ofone of the plaques confirms the suspecteddiagnosis of psoriasis.
Cardiology
Latest News
Advertisement
Advertisement
A middle-aged man with"jock itch" that has failed torespond to antifungal creams.An older woman who has diffusehyperkeratosis of predominantlyweight-bearing surfaces.A young man with mildlypruritic, small, salmon pinkpapules and thick white scaleon his trunk and arms.
A 30-year-old man presents with scalingand erythema of the scalp that extendspast the anterior hairline. Thepatient has a family history of psoriasis.For the past 5 years, he has experiencedwintertime flares of the diseasethat affect his scalp and the extensorsurfaces of the extremities.
A 46-year-old man complains that his"jock itch" failed to respond to antifungalcreams. The patient has hadpsoriasis on his elbows and knees formany years.
A 72-year-old man presents with skinlesions and nail abnormalities. Erythematous,sharply defined, demarcatedpapules and rounded plaquescovered by silvery micaceous scaleare noted on the elbows, knees, andscalp. Involved areas appear to be bilaterallysymmetric. Localized psoriasisvulgaris is diagnosed.
4A:Small, slightly pruritic, salmonpink papules with thick white scalehave arisen over the past 5 days onthe trunk and arms of a 24-year-oldman. The patient has a history ofvery mild psoriasis vulgaris of the elbows,knees, and scalp; he deniesstreptococcal pharyngitis or other recentinfections. Guttate psoriasis isdiagnosed.
Focal, painless discoloration of theleft thumbnail (A) developed severalyears earlier in this 46-year-old man.Oral antifungal therapy had no effecton the lesion.
A 35-year-old man presents with extensiveplaques over much of thetrunk and extremities. This severeflare of psoriasis developed after astressful emotional experience.
A 60-year-old man with a long historyof psoriasis vulgaris required a systemiccorticosteroid for a severe exacerbationof asthma. Soon after theErythrodermic or Pustular Psoriasiscorticosteroid was discontinued, generalizederythema and scaling of theskin developed.

A 67-year-old woman, who had hypertension and chronic obstructive pulmonary disease, presented to the emergency department with mild abdominal discomfort and shortness of breath.

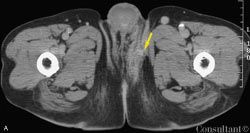
A 40-year-old man presented with a 5-year history of progressively increasing bilateral leg swelling that was neither painful nor pruritic. There was no history of dyspnea, jaundice, or groin surgery. The patient reported multiple previous episodes of superimposed cellulitis, which were treated with antibiotics. There was no family history of similar illness.
For several days, a 60-year-old woman has had fever, myalgias,fatigue, poor appetite, and diminished oral intake. Shedenies cough, sputum production, and urinary symptoms.

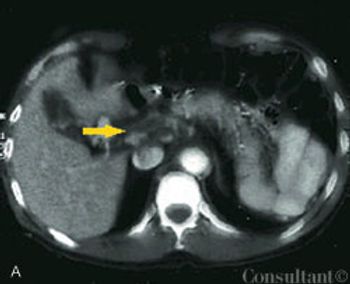
A 75-year-old man was brought to the emergency department with fever, cough, and abdominal pain of 2 days’ duration. The pain was most severe in the epigastric and umbilical regions. The patient’s history included type 2 diabetes mellitus, hypertension, and hypercholesterolemia. He had smoked cigarettes for 40 years and recently lost 50 lb. The patient was tachypneic and diaphoretic.
The Geriatric Depression Scale is the most widelyvalidated screening tool. The questionnaire has beenreduced to a single question that is as sensitive and as specificas the 15-item shortened form of the original 30-itemscale. The question is: "How often do you feel sad or depressed?'This is certainly something that is easy to ask inthe course of a general physical examination or routine officevisit.
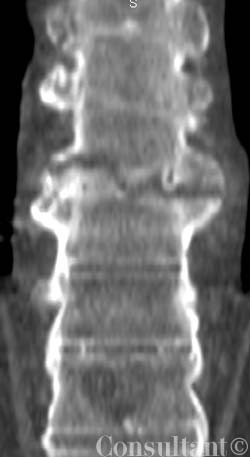
A 60-year-old man presented to the emergency department (ED) with fever of 1 day’s duration and midabdominal pain. The cramping pain had begun 3 days earlier in a bandlike distribution around the upper abdomen. Ingestion of food exacerbated the discomfort. The patient had a history of intermittent constipation; he denied alcohol or illicit drug use, nausea, vomiting, and weight loss. He did not use any herbal or over-the-counter medications.

A 40-year-old man presented to the emergency department with moderate to severe pain over the left lateral wrist. Earlier in the day, an iron rod had accidentally struck his wrist. The patient’s history included chronic obstructive pulmonary disease, hypertension, and social anxiety disorder.
A network of purplish pink lesions recently developed on a 28-year-old woman’sarms and legs. The asymptomatic rash becomes more prominent with exposureto cold. The patient denies fever, aches, arthralgias, oral erosions, chestpain, and photosensitivity.
Three weeks after coronary artery bypass graft (CABG)surgery, a 52-year-old woman complained of pain at thesternal scar. The patient had a history of diabetes and hypertension.She had smoked cigarettes for many years.

A 72-year-old woman presented to the emergency department with epistaxis and generalized telangiectasia. The patient was known to have Rendu-Osler-Weber syndrome, or hereditary hemorrhagic telangiectasia, an autosomal dominant disorder that is associated with arteriovenous fistulae of many organs.

In a 65-year-old man with a family history of colorectal carcinoma, an initial screening coloscopic examination revealed 2 arteriovenous malformations. These delicate red lesions with a vascular network and irregular edges were found in the cecum.
Many patients who present to the emergency department(ED) with severe headache request a narcotic to relieve thepain.

A 59-year-old woman presented for a routine physical examination. She had no physical complaints and took no medications. During the physical examination, bilateral, flat, slightly elevated, yellowish cutaneous lesions were noted above and below the skin folds of the patient's eyelids.
A 54-year-old man is admitted to the hospital because of worsening lower extremityswelling and knee and ankle pain and stiffness. These symptoms havemade walking very difficult for the past month.
The family of a 50-year-oldalcoholic man brings him to youroffice. They are concerned abouthis health and note that they had notseen him for several months beforehe reappeared. The patient complainsof generalized weakness, fatigue, andbleeding gums.
For the past several weeks, a 54-year-old man has had progressivelyworsening abdominal pain and general achiness.He has no nausea, vomiting, diarrhea, or fever and no historyof trauma.
Advertisement
Advertisement
Trending on Patient Care Online
1
From Amyloid Clearance to Daytime Function: Why Sleep Quality Matters for Brain Health
2
FDA Approves First Oral PCSK9 Inhibitor to Reduce LDL-C in Adults With Hypercholesterolemia
3
FDA Accepts Cefiderocol sNDA for Pediatric Gram-Negative Infections
4