






























































































































































A 56-year-old woman was referred for management of severe hyperlipidemia. Her family history included hypercholesterolemia and premature coronary artery disease.

A 56-year-old woman was referred for management of severe hyperlipidemia. Her family history included hypercholesterolemia and premature coronary artery disease.

Cutaneous manifestations develop in approximately 30% of persons with diabetes. Premature atherosclerosis is a common complication of the disease that can cause peripheral infarction, ulceration, and necrosis.
A serum alkaline phosphatase (ALP) level three times higher than normal, found on routine laboratory examination, prompted further evaluation of a 57-year-old man. At admission, his temperature was 36.8°C (98.2°F), blood pressure was 120/85 mm Hg, pulse rate was 90 beats per minute, and respiration rate was 19 breaths per minute. The physical examination was unrevealing, and the patient's personal and family medical histories were unremarkable.

Atropy of the paravertebral musculature--the "spine sign"--in this 64-year-old man offers clues to the genesis of the coronary artery disease for which he had undergone a coronary artery bypass graft (CABG) and to the cause of his severe post-CABG anterior chest pain.
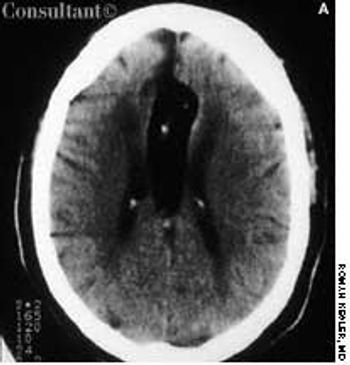
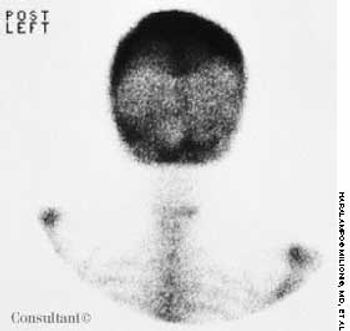
A 62-year-old African American woman was brought to the emergency department (ED) after the sudden onset of slurred speech and weakness in her left arm and leg. Her medical history included hypertension, insulin-dependent diabetes, and congestive heart failure.

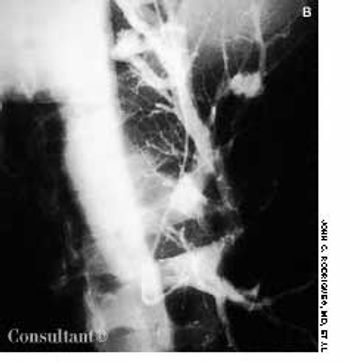
A 56-year-old man, who had a history of cigarette smoking, noticed a sudden swelling in his neck, mainly on the right side. Shortly thereafter, his right arm became enlarged.

This rare condition affects both men and women. The average age at onset is 53 years. The lesions are deep brownish red to purple papules, nodules, and plaques. Blisters and ulcers also can occur.

Relapsing polychondritis, as manifested in one of this 55-year-old man's deformed ears, is a rare, chronic, autoimmune inflammatory disease of cartilaginous structures. The disease also affected the cartilage in this patient's nose, which is the second most common site of involvement. Tissues of the joints, eyes, and blood vessels as well as the trachea and the bronchial tree may also be affected and destroyed.
A 72-year-old woman presented for her annual physical examination. She had been treated for tuberculosis 20 years earlier. The patient did not smoke cigarettes; she denied fever, chills, and rigors.

A 36-year-old man was admitted to the hospital with acute mid-epigastric pain and vomiting. He was a heavy drinker and had smoked between 50 and 60 cigarettes a day for the last 15 years.

Frequent urinary tract infections and unexplained hypertension (160/100 mm Hg) occurred in a 38-year-old man with no significant medical history. The heart and chest were normal; a right lower quadrant mass was detected in the abdomen. Red blood cells were found in the urine. An abdominal CT scan demonstrated that the left kidney was fused to the lower pole of the right kidney with the left pelvicaliceal system to the left of the midline; these findings are consistent with crossed fused renal ectopia. Cystographic and cystoscopic examinations were normal.

A 35-year-old man, a smoker, had right pleuritic pain, productive cough, and fever for 3 days. His pulse rate was 107 beats per minute; respiratory rate, 14 breaths per minute; blood pressure, 136/80 mm Hg; and temperature, 37.7°C (99.9°F). There were signs of right upper lobe consolidation. Laboratory studies showed hyponatremia. Chest films showed a homogeneous density in the right upper lobe.

A 71-year-old man, who had recently returned from a month in Europe, complained of left lower leg swelling and pain of 1-week's duration. For many years, this obese patient had chronic venous insufficiency of both legs and chronic osteoarthritis of the knees that severely limited his ability to walk. The patient was admitted to the hospital with extensive cellulitis of the left lower leg.

This 8-year-old girl presented with bilateral ptosis, down-slanting palpebral fissures, malar hypoplasia, mild micrognathia, and mild webbing of the neck. She also had marked lumbar lordosis and a dextroconvex thoracic scoliosis with scapular winging. There was a generalized reduction in muscle mass with proximal limb weakness, short stature, diminished deep tendon reflexes, and an awkward waddling gait.

A 61-year-old woman who was receiving dialysis for diabetes-associated end-stage renal disease was hospitalized for care of an abdominal wound that had been debrided and closed. At this time, the patient had several large, indurated, red plaques with central, stellate, black eschars on her abdomen, left buttock, and legs. An early focus of ulceration was noted superior to the stapled incision.
Having suffered progressive shortness of breath for 2 years, a 35-year-old man was eventually hospitalized. The patient's dyspnea had worsened over the past year, but he had neither chest pain nor palpitations. His primary care physician first noticed finger clubbing 8 months ago.

A 41-year-old man complaining of left-sided chest pain for 2 hours was examined in the emergency department (ED). On arrival, his blood pressure was 160/100 mm Hg; heart rate, 90 beats per minute; respiratory rate, 18 breaths per minute; oxygen saturation, 99%; and temperature, 37.2°C (99°F).

Police brought a delirious, combative 24-year-old man to the emergency department. The patient was unable to provide any history on arrival, but his scarred, blistering lips and his vital signs (blood pressure, 166/102 mm Hg; heart rate, 97 beats per minute; respiratory rate, 24 breaths per minute; and temperature, 38.2°C, or 100.9°F) led to a possible diagnosis of cocaine-induced delirium.

An 80-year-old woman presented with recurrent abdominal pain for 1 month, constipation, and vomiting. She had no diarrhea, rectal bleeding, or weight loss.

A 49-year-old woman with a history of alcoholic cirrhosis, esophageal varices, coronary artery disease, diabetes mellitus, and hypertension presented to the emergency department with a 2-day history of fever, chills, nausea, and back and abdominal pain. The pain began on the right side, progressed to the lower back, and radiated into the right anterior thigh and groin area.

A 52-year-old man from Bangladesh had suffered from pleuritic pain for 1 week. He had never had tuberculosis and-except for being a cigarette smoker-had no notable medical history. The only remarkable findings were a temperature of 37.5°C (99.5°F) and anterior tenderness over the right lower rib cage. Laboratory test results were normal. A tuberculin test with 5 TU of purified protein derivative produced positive results, with a 15 × 17-mm induration.
A 63-year-old man was given oral celecoxib, 100 mg bid, for shoulder pain. Three days later, a pruritic rash appeared on his back, then spread to the chest, lower legs, and face. He stopped the celecoxib on his own and self-administered diphenhydramine for the pruritus. The rash and itch persisted, which prompted the patient to seek medical care. He had no respiratory symptoms.

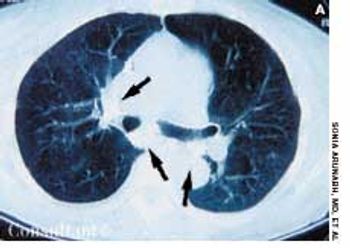
A 45-year-old man with a history of congestive heart failure presented with cough and dyspnea. A chest roentgenogram showed loculated pleural effusion in the horizontal fissure of the right lung, and a CT scan revealed pleural-based density in that lung.

A 19-year-old man was admitted to the hospital with malaise, fatigue, and intermittent fever (temperature of 38°C [100.4°F]) for the last 2 weeks. Physical examination revealed scarce purpuric lesions over the lower extremities; a pericardial friction rub was audible over the precordium when the patient was supine and seated, and the spleen was remarkably enlarged.

Levofloxacin, 500 mg/d, had been prescribed for a 74-year-old woman who had a urinary tract infection. The patient had type 2 diabetes and hypertension. She was allergic to sulfa drugs.