





























































































































































A 36-year-old man was admitted to the hospital with acute mid-epigastric pain and vomiting. He was a heavy drinker and had smoked between 50 and 60 cigarettes a day for the last 15 years.
A 36-year-old man was admitted to the hospital with acute mid-epigastric pain and vomiting. He was a heavy drinker and had smoked between 50 and 60 cigarettes a day for the last 15 years.

A 61-year-old woman who was receiving dialysis for diabetes-associated end-stage renal disease was hospitalized for care of an abdominal wound that had been debrided and closed. At this time, the patient had several large, indurated, red plaques with central, stellate, black eschars on her abdomen, left buttock, and legs. An early focus of ulceration was noted superior to the stapled incision.

A 63-year-old woman who was on long-term hemodialysis because of diabetic end-stage renal disease had a 7-month history of waxing and waning papules and plaques on the front of both legs. The asymptomatic multiple, discrete, slightly erythematous, round to oval lesions ranged from 5 mm to 3 × 4 cm. Several had heaped-up borders and contained central crust and keratotic debris; others were superficial ulcers with central eschars. The lesions improved only slightly following twice-daily application of a superpotent topical corticosteroid preparation.
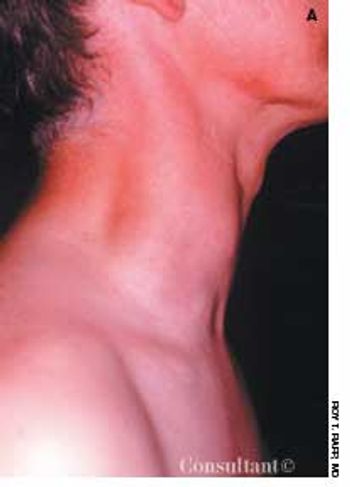
A 40-year-old man was concerned about an enlarging painless mass on the right side of his neck that had been present for 6 months. The patient reported no other health problems; his medical history was unremarkable, and he was taking no medications.

Two days of pain in his right leg, which had been swollen for a week, brought this 69-year-old man with type II diabetes to the emergency department (ED). Three months earlier, the patient had undergone a radical retropubic prostatectomy with bilateral pelvic lymph node dissection. Examination in the ED revealed an edematous right leg indurated with a leathery-appearing thigh that was hot to the touch. His temperature was 38.7°C (101.7°F), and his white blood cell count was 21,290/µL with a shift to the left.

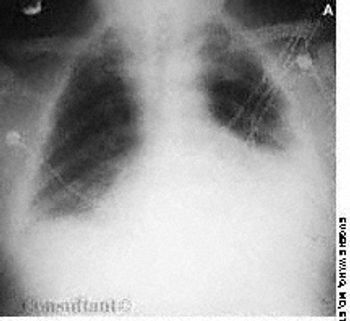
A 69-year-old woman was admitted to the hospital with wheezing and dyspnea. She also complained of hoarseness and slight dysphagia that had caused a loss of 12 lb during the past 4 months. The patient had been treated for bronchial asthma as an outpatient, but the worsening episodes of wheezing were not being controlled by bronchodilator therapy.

An 80-year-old woman presented with recurrent abdominal pain for 1 month, constipation, and vomiting. She had no diarrhea, rectal bleeding, or weight loss.

A 49-year-old woman with a history of alcoholic cirrhosis, esophageal varices, coronary artery disease, diabetes mellitus, and hypertension presented to the emergency department with a 2-day history of fever, chills, nausea, and back and abdominal pain. The pain began on the right side, progressed to the lower back, and radiated into the right anterior thigh and groin area.

A 32-year-old man presented with a yellow, papular rash on the buttocks and extensor surfaces. His medical history included diabetes mellitus, alcoholism, obesity, and polysubstance abuse. Laboratory results disclosed a serum triglyceride level of 5,793 mg/dL.

Two years ago, Dr Alexander K. C. Leung reported on a case of pseudopseudohypoparathyroidism. The patient was a 13-year-old girl with short stature, short fourth metacarpals and metatarsals, mild mental retardation, and no identifiable biochemical abnormalities.

A 24-year-old woman was concerned about a protruding epigastrium mass that had grown since it was first noted 4 months earlier. She had no abdominal pain, nausea, or vomiting.
The persistent effects of Graves disease were evident in a 48-year-old woman who had recently emigrated from Haiti to the United States. Thyrotoxicosis had developed several years before she sought treatment in her native country. The patient's obstructive goiter was removed and treatment with thyroxine was begun.

Levofloxacin, 500 mg/d, had been prescribed for a 74-year-old woman who had a urinary tract infection. The patient had type 2 diabetes and hypertension. She was allergic to sulfa drugs.

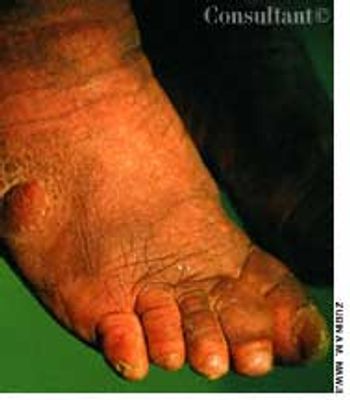
A 73-year-old man was admitted to the hospital with pain in his hands, feet, and elbows. The patient, an alcoholic, had a 20-year history of hypertension and diabetes. Deformities of the hands and feet had developed during the past 5 years. Tophi were present over both ear lobes. The serum uric acid level was 15 mg/dL.

This 14-year-old boy presented with slowly progressive hypopigmented lesions that had been present on the lower extremities for the previous 2 years.

A 45-year-old man sought medical advice after suffering for 6 months with recurrent pain and a purulent discharge at the sacrococcygeal region. Two weeks before this consultation, an abscess on the patient's right buttock had been drained by another physician. The patient had insulin-dependent diabetes mellitus for 5 years; his medical history was otherwise unremarkable.
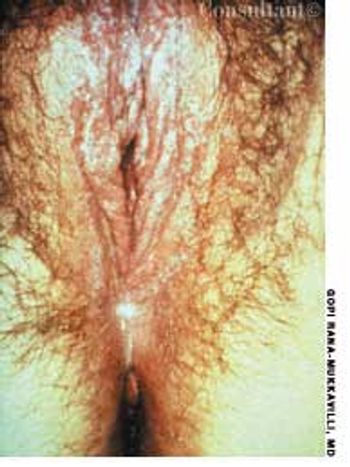
For 3 days, a 23-year-old woman had been bothered by pruritic vaginal and vulvar lesions. A cheesy white vaginal discharge was associated with the itching.

A 79-year-old nursing home resident was hospitalized for evaluation of hyperkalemia and leukocytosis. Her medical history included hypertension, respiratory failure with subsequent tracheostomy placement and ventilator dependency, and anemia. Both of her legs had been amputated above the knee secondary to complications of type 2 diabetes mellitus.

Concerned about a lesion between her eyes, a 91-year-old woman sought medical evaluation. She had not seen a physician for 23 years.

A boy was born to a gravida 2, para 1, 26-year-old woman at 37 weeks' gestation. The pregnancy had been complicated by gestational diabetes.

A 10-year-old boy presented with a 6-month history of a painless mass on the left side of the scrotum. The overlying skin had a bluish discoloration. The mass felt like a “bag of worms.” When the boy stood, venous varicosity could be palpated along the spermatic cord. This venous distention increased when he performed Valsalva's maneuver and decreased when he was recumbent.
A 76-year-old man reported a 3-month history of an asymptomatic, raised, reddened lesion on his penis. The patient had type 2 diabetes mellitus. In 1994, a basal cell carcinoma had been excised from his chest and, 3 years later, a squamous cell carcinoma was excised from his left temple.

A 44-year-old woman was being seen regularly for skin manifestations of systemic lupus erythematosus (SLE). During a routine visit, blotchy erythema and hyperpigmentation were noted on the normally exposed areas of her neck and upper chest; the submental area was spared. Close examination revealed fine telangiectases and poorly marginated hyperpigmented and hypopigmented macules.

Severe pain in the scrotum during a soccer game sent a 14-year-old boy to his physician. The right testicle was swollen and exquisitely tender. On exploration, it was hemorrhagic and blue-black. A small incision in the tunica of the testis revealed arterial bleeding, which indicated that the testis was still viable. The right testicle was untwisted and fixed to the scrotum.
Over the previous 6 months, a 59-year-old man had experienced lethargy, fatigue, poor appetite, cold intolerance, and abdominal distention. His vital signs were normal; physical examination revealed periorbital and pretibial edema, distant heart sounds, and delayed reflexes.