





























































































































































A 57-year-old man was brought to the emergency department with fever, chills, and a productive cough of 1-week's duration. He had a history of alcoholism.
A 57-year-old man was brought to the emergency department with fever, chills, and a productive cough of 1-week's duration. He had a history of alcoholism.

A mildly painful, nonpruritic rash on the forearms and legs prompted a 42-year-old man to go to the emergency department (ED). The patient noted the rash when he awoke that morning. He had had joint pain and fever for the past 7 days and generalized malaise with chills that began about 3 days earlier. He had no significant medical history.

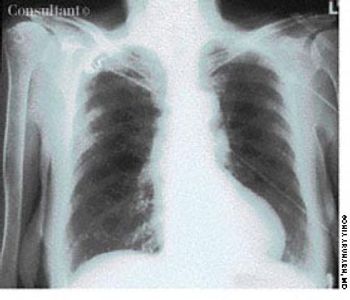
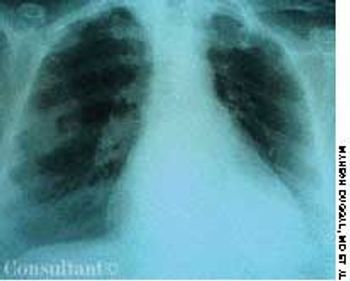
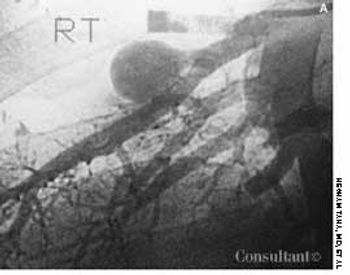
A previously healthy 51-year-old man presented with weight loss and poor appetite of 2 months' duration. He was heterosexual and had many sexual partners. Except for a temperature of 38.3°C (100.9°F) and left basal rhonchi, results of physical examination were normal. A chest radiograph and CT scan, as seen here, showed large cavitary lesions in the lower left lobe.
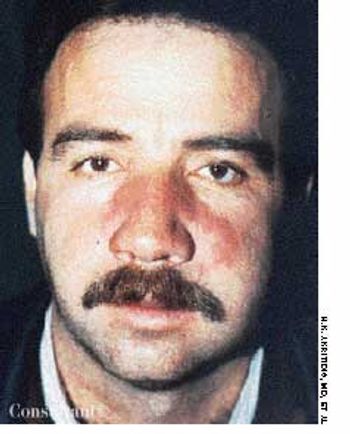
A 40-year-old man was hospitalized with the superficial, reddening, and painful facial lesion seen here. Its borders were sharp, and it had developed rapidly. The patient had a temperature of 40°C (104°F) and chills. His erythrocyte sedimentation rate was elevated, and he had neutrophilic leukocytosis.
A 40-year-old man, originally an Ohio resident, underwent a chest x-ray study during medical clearance following surgery to repair a hernia. Although the patient had no pulmonary symptoms, the film showed multiple small, punctate calcifications in both lung fields.
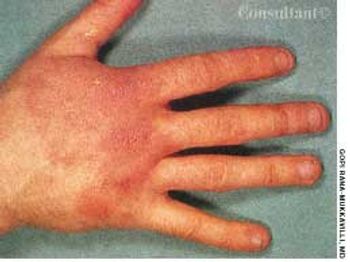
After 1 week of scratching a pruritic, reddish rash on a swollen hand and enduring a “burning sensation,” a 43-year-old man visited his physician. The patient worked as a meatpacker. He had no other medical conditions, took no medications, and had no known drug allergies.

An afebrile 23-year-old man with no cervical gland enlargement presented with the very painful, large, shallow, yellowish-based ulcer shown here.
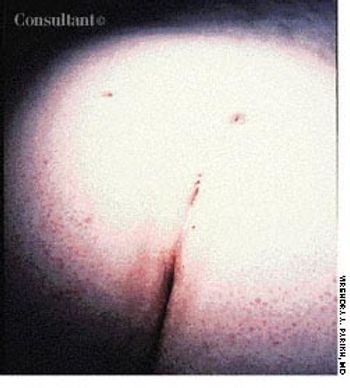
Pain, swelling, and purulent, blood-stained drainage around the lower back had plagued a 21-year-old woman for 3 weeks. On examination, multiple openings were seen overlying the natal cleft, the sacrococcygeal region, and the upper part of the midline. The last was the area of drainage. Insertion of a metal probe at that point revealed a pilonidal sinus that communicated with centrally located openings.
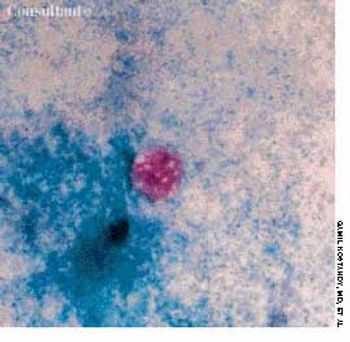
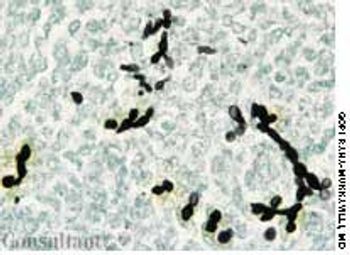
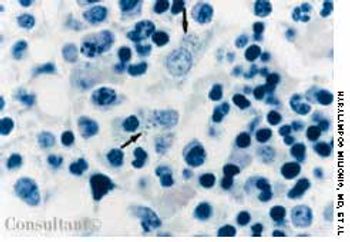
A 32-year-old Hispanic woman with AIDS presented with a 1-month history of diarrhea; abdominal bloating and cramps; loss of appetite; and pronounced fatigue, malaise, and weight loss. She had no fever or chills and was not vomiting. Her CD4+ cell count was 12/µL. Results of a routine microscopic examination of stool for ova and parasites were negative; an acid-fast stain of stool demonstrated oocytes of Cyclospora cayetanensis measuring 8.8 mm in diameter (pictured, magnification ×1,000). This is about twice the size of the Cryptosporidium parvum oocyte, which typically is 4 to 5 mm.

After suffering with a severe, disabling headache for 2 weeks, a 20-year-old soldier sought medical treatment. He had no significant medical history other than his 6-year history of smoking.
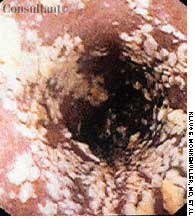
A 72-year-old nursing home resident was hospitalized with fever, chills, and rigors of 2 days' duration. The nursing home staff reported the patient had dysphagia after a recent stroke.

Following an uncomplicated pregnancy, a 30-year-old gravida 2, para 1 mother delivered a term infant boy. The neonate's Apgar scores were 7 at 1 minute and 9 at 5 minutes. Birth weight was 3.2 kg (7.1 lb); length, 50 cm (19.7 in).

Erythematous, scaly lesions with double-edged borders had been present on a 14-year-old boy's left upper arm and lower legs for about a year. The lesions were occasionally pruritic, and some resembled ringworm. At times, fine yellow crusting suggestive of impetigo was present. The boy took very hot baths and showers.
Fever occurring twice daily, accompanied by profuse sweating, anorexia, and malaise of 15 days' duration resulted in hospitalization of a 31-year-old woman. At this time, her temperature was 37.6°C (99.7°F); blood pressure, 110/70 mm Hg; pulse rate, 90 beats per minute; and respiratory rate, 18 breaths per minute. A palpable spleen was about 3 to 5 cm below the left subcostal margin. Neither lymphadenopathy nor hepatomegaly was noted.

An eruption on the face of a 49-year-old woman had been misdiagnosed as a staphylococcal infection; the rash failed to respond to oral and topical antibiotics. A mid-potency topical corticosteroid also had been tried, but the eruption worsened.
A 22-year-old man complained of progressive shortness of breath and abdominal distention. Three years before, he had completed chemotherapy for Hodgkin's disease and had since been in remission. Recently, he had been treated for tonsillitis with oral antibiotics.

An otherwise healthy 36-year-old woman complained of multiple tender, hot, bright red nodules of acute onset on her thighs and anterior tibial areas. Antibiotics had been given for a suspected infection, but the rash persisted.

The widespread eruption of asymptomatic macules and flat, palpable, flesh-colored lesions prompted a 23-year-old woman to consult her physician. The lesions-some of which had dark centers-were concentrated on the patient's face, neck, and upper back; the palms, soles, anal mucosa, and genital areas were clear. The patient denied systemic symptoms. She was seronegative for HIV.

A papule on the leg of an 11-year-old boy had suddenly developed into a slightly tender pustule. The pustule had not responded to oral cephalexin and topical mupirocin prescribed by another clinician.

Two 7-year-olds show the purpuric rash of the lower body and legs that is typical of Henoch-Schönlein purpura. This disease is a vasculitis that chiefly affects small vessels of the skin, joints, gastrointestinal tract, and kidney.

A 52-year-old white man presented with a pruritic eruption on the neck of 3 months' duration. The rash had not responded to a potent topical corticosteroid prescribed by another practitioner for the presumed diagnosis of eczema.

A 13-year-old girl who had leukemia presented to the emergency department with fever; chills; weight loss; fatigue; and a painful, erythematous rash with a central black lesion on the upper thigh. The patient was neutropenic and had been undergoing chemotherapy for 1 week.

A healthy 31-year-old man was referred to a dermatologist with a diagnosis of tinea versicolor that did not respond to oral ketoconazole and topical selenium sulfide.

Shortly after arriving from Puerto Rico, a 59-year-old man presented with right-sided frontal head pain and decreased vision in his right eye. He was concerned about a “sore” that first developed 9 months earlier on his head. The patient denied fever, chills, and syncope.

The wounds on the back of this boy's head are the result of an encounter with his neighbor's dog. The youngster's anxious parents brought him in for evaluation 1 hour after he was bitten.